
Clinical Application of an Abusive Practice is Still Abuse
The JRC is getting away with torture disguised as treatment
Cognitive dissonance
At the end of May, the Association for Behaviour Analysis International (ABAI) held their annual convention.
An issue which has garnered a lot of attention recently — or once again, as it’s been an issue for more than a decade — is the use of electric skin shock on disabled and Autistic people at the Judge Rotenberg Centre (JRC) in the U.S.
Applied Behaviour Analysis (ABA) is the approach used at JRC, with electric skin shock being used as an aversive to punish disabled and Autistic people for unwanted behaviours.
It is a barbaric form of torture in all cases, but in this case it is particularly heinous, because electric shock is being used on vulnerable people as a means of controlling their behaviour and forcing compliance.
Advocates for, and self-advocates in, the disabled and Autistic communities have pressured ABAI and related organizations to come out in strong opposition against the use of electric shock on human beings.
Seems like a no-brainer, right?
Apparently not.
It’s not a trick question
Instead of immediately coming out against the torture of disabled and Autistic people, ABAI assembled a task force. Yes, a task force to discuss the pros and cons of shocking disabled and Autistic people.
NeuroClastic, a non-profit self-advocacy organization run by Autistic and disabled adults, has shared the transcript from a forum held at ABAI’s recent conference. A forum to discuss the use of electroshock.
I will share a few of ABAI’s forum questions below, along with my own comments and answers.
How is skin shock used in contemporary behaviour analysis?
Literally speaking, JRC allows their staff to place an anklet on residents — similar to shock collars used on dogs, but using higher voltage.
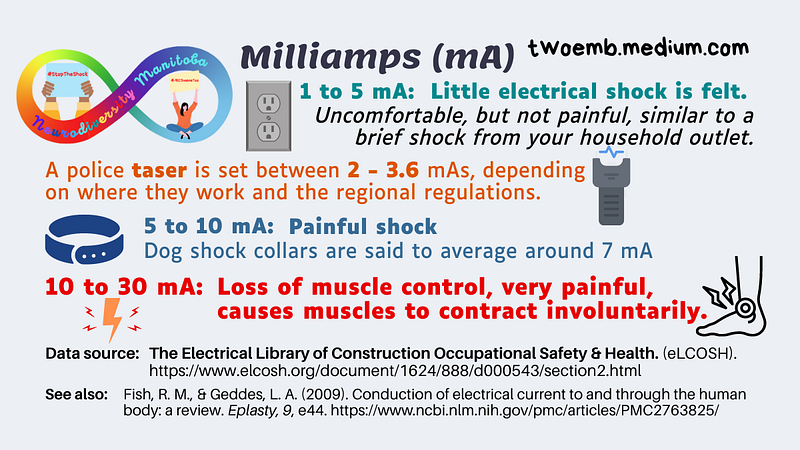
When the individual engages in behaviour deemed by JRC staff to be “inappropriate”, staff can administer an electric shock to the person’s body.
Philosophically speaking, given what we now know and understand about how stress impacts one’s cognitive capabilities and the negative health impacts of prolonged stress, one can easily say there is no place for such practices in modern society.
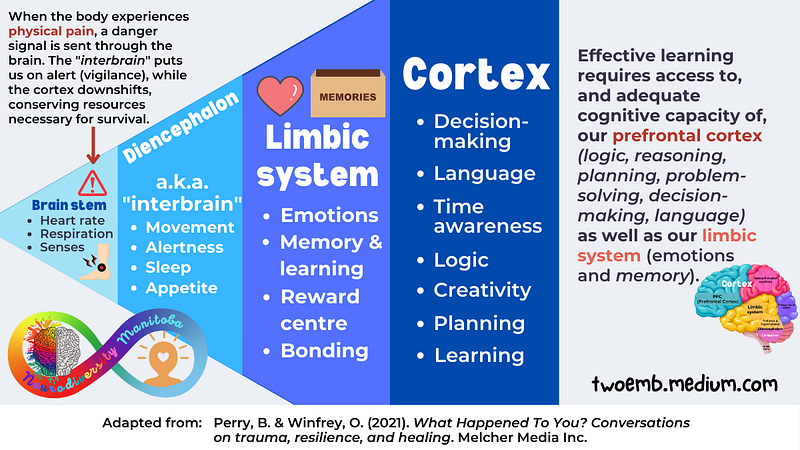
To put it simply: stress, pain, and fear all inhibit learning. Inflicting physical pain, however “mild” JRC wishes to describe it, causes the brain to go into flight-or-flight mode.
The brain redirects resources from our cortex (responsible for important functions such as reasoning, logic, decision-making, and problem-solving) to the areas of the brain needed for survival. This is why we cannot think clearly when we panic or are experiencing intense emotions.
What are the best practices for implementing it and fading it out of a treatment plan, or removing it all together?
Treating disabled and Autistic people like human beings would be a good start. Next would be:
- Provide effective modes of communication, as required to meet the unique needs of each individual (“inappropriate” behaviours are often attempts at self-regulation or attempts to communicate).
- Meet people’s sensory, emotional, and environmental needs. Often dysregulation happens due to sensory overload, overwhelm, or not having other needs met. If these were the priorities, rather than modifying people’s behaviour like lab rats, they’d be providing support rather than inflicting distress and torture.
- Teach skills in a way that respects the autonomy of each person, and respects their emotional, sensory, and environmental needs. This means focusing on skills necessary and important to that individual, not as determined by neurotypical staff or family members.
- Presume competence. Non-speaking does not mean non-thinking or non-communicating. It’s not okay to abuse and torture people simply because you haven’t figured out a way to effectively communicate with them.
- Respect each person’s neurotype and individuality. The goal isn’t to “train” a human being to become more neurotypical, the goal is to provide accommodations and supports as necessary for that person to be themselves and pursue their own interests.
What ethical issues are raised by skin shock that distinguish it from the alternatives?
Anything that inflicts fear, pain, distress, or intentionally causes a person discomfort, is ethically and morally wrong. Plain and simple.
Cognitive dissonance
The ABAI’s forum included the following statement:
“In this context, we understand skin shock to be a narrowly focussed, clinical application of an operant punishment procedure. In this sense, it is distinguished from other aversive methods such as conventional corporal punishment and conversion therapy which have been condemned by the association.” — Association for Behaviour Analysis International
Clinical. Application.
The definition of clinical is “involving or relating to the direct medical treatment or testing of patients”. Application is “the action of putting something into operation.”
ABAI is defining the electric shock of Autistic and disabled people as a form of medical procedure or treatment, thus distinguishing it from corporal punishment, which is defined as “a physical punishment which is intended to cause physical pain to a person.”
Punishment is something which reduces or stops a behaviour. Punishment which causes pain is considered corporal — corporal meaning “relating to, or affecting the body.”
Not to overwhelm you with definitions, but I want to clarify one last highly relevant term. Cognitive dissonance is a “psychological conflict resulting from incongruous beliefs and attitudes held simultaneously.”
Because electric skin shock has historically been either endorsed or ignored by ABAI and similar organizations, this somehow qualifies it as a “therapy” or “treatment”, simply because they’ve used it under this guise.
When a person experiences cognitive dissonance, there are a few ways they can relieve this discomfort:
- Reject, explain away, or avoid the new information
- Reconcile the differences (i.e. change their beliefs or behaviour)
- Resort to any other defensive means of preserving stability or order in their conceptions of the world and of themselves.
It appears ABAI is choosing option #3.
© Jillian Enright, Neurodiversity MB

When you join medium, as a member you’ll have access to unlimited reads for only $5 per month. If you use my referral link, I’ll earn a small commission, and you’ll earn my undying gratitude.



