
Rethinking Rejection Sensitive Dysphoria (RSD)
The feelings are real, but they got the cause all wrong

Rejection sensitive
You may have heard this term going around, referring to something called “Rejection Sensitive Dysphoria”, or RSD.
There are a number of possible reasons those of us with ADHD experience emotions more intensely than others. We often struggle with emotional lability, emotional impulsivity, emotional dysregulation, and negative intent attribution.
This has led to a lot of discussion about the term Rejection Sensitivity Dysphoria (RSD) in the ADHD community over the past few years. The detailed descriptions of what RSD feels and looks like resonate with so many people who also have ADHD.
I even wrote an extensive piece about it in the summer.
However…
Did you know that RSD is not in the DSM-V, nor is it recognized in the psychiatric or psychological communities?
Don’t get me wrong, people don’t need their experiences to be medicalized in order for them to be 100% real and valid. It can be extremely validating to have our feelings put into words and to find out that so many others have similar experiences.
The description of RSD is very real, as an overwhelming majority of the ADHD population can attest to, which is why I was so drawn to exploring and researching it in the first place.
People don’t need their experiences to be pathologized in order for them to be entirely real and valid.
But now I want a do-over because I’ve learned a lot more and, as a result, have some important things to add. Notably, the fact that RSD is attributed to ADHD and neurodivergence has me thinking about this whole concept more critically.
There is very little actual research done on Rejection Sensitive Dysphoria (read: none), so it’s very difficult to critique research that doesn’t exist.
RSD is a term made up by Dr. William Dodson to describe the experience of many of his ADHD patients. In fact, he claims an alarming 99.9% of his patients experience RSD and cites it as their biggest problem, a figure for which the doctor provides zero data.
The primary information about RSD is available on the ADDitude Mag website and on Dr. Dobson’s own website, neither of which cites any peer-reviewed research. Dr. Dobson’s website has zero citations, and ADDitude Mag’s website only cites itself and takes you in circles around other articles on their website.
Dr. Dodson took old descriptions of atypical depression from an “old psychiatric textbook” (specific source not provided), which had cited RSD as part of a mood disorder.
Dr. Dodson instead says that RSD is directly caused by ADHD.
At least he does acknowledge that criticism is a common experience in the lives of people with “unrecognized and untreated ADHD”, yet says nothing about the very real and continued criticism many of us experience after ADHD is diagnosed and treated.
It’s not disordered when it’s a rational response to actual repeated rejection
Research has shown that children diagnosed with ADHD are, in fact, more often rejected by their peers. As many as 52% of 7–9 year old children with ADHD fall in the rejected category.
Children with ADHD are also more vulnerable to bullying and victimization, and many adults with ADHD describe childhood experiences of rejection and bullying by peers.
Dysphoria comes from the Greek words dys (pain) and pherein (to carry), also loosely translated as “pain which is hard to bear”. Dr. Dodson’s website provides the following description:
Rejection-Sensitive Dysphoria is often experienced as if it were a physical wound. Patients will hunch over and clutch their chests as if they have just been stabbed... If they internalize the pain they can instantaneously drop into a full Major Depression-like syndrome.
Well, if you spent a significant part of your childhood experiencing actual rejection, criticism, and bullying, it stands to reason that you would become hypersensitive to these experiences.
“Personal identities are constituted through their relationship to the world in regard to self-image, self-esteem, individuality, and social position within society.”
— Alan Jurgens
It makes sense that so many of us have more intense reactions to rejection compared to those who have grown up feeling accepted and appreciated — those who had the environment and circumstances in which to develop a healthy sense of self.
The social model
Where the pathology paradigm asks “what is wrong with the individual?”, the social model of disability asks, “what’s wrong with the person’s environment?”
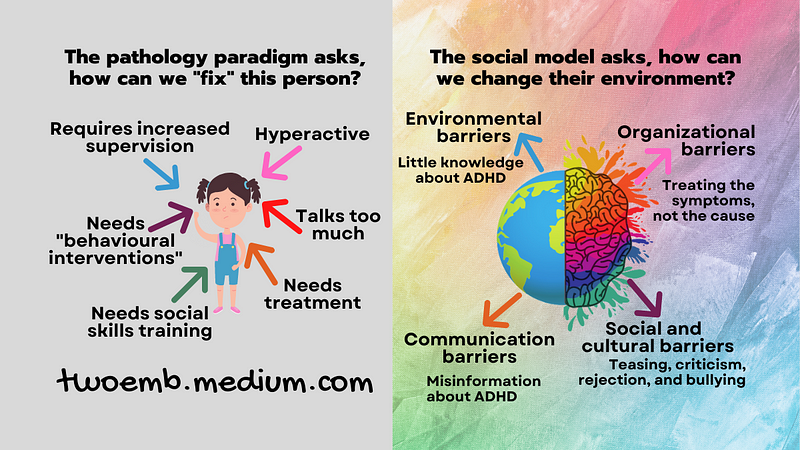
“Social attitudes are a key component in the dynamics of enablement and disablement.”
— Dr. Nick Walker
When a person encounters difficulties, the social model does not ask what is wrong with the person. Instead, this model points to the context and surrounding environment.
The social model seeks to uncover and change how institutions and cultural norms disable individuals due to a lack of understanding, acceptance, and accommodation.
As it relates to RSD, rather than blaming the neurodivergent individual for a reasonable response to experiencing undue criticism, rejection, and bullying, we should instead look at how and why people are mistreating someone simply because they are different.
As Dr. Dodson even says,
“RSD is always triggered by some event and because the mood shift matches the nature of the trigger, the internalized RSD can be considered a normal mood in every way except its intensity.”
So the good doctor acknowledges that there’s been some kind of upsetting event, but perhaps the individual’s reaction was so intense that it causes them great distress.
Rather than recommending medications like guanfacine and clonidine, which Dr. Dodson does on the ADDitude website, perhaps we could address the complex trauma stemming from so many painful experiences.
Giving someone a medication that was originally formulated as treatment for high blood pressure in order to reduce their impulsive responses may help quell the intensity of their emotions but will do nothing to change the external environment in which they continue to experience real rejection.
I’m also not anti-medication, I’m a proponent of good healthcare, but I dislike bandaid solutions. I hate gaslighting and victim-blaming even more.
I’m not saying that we, as neurodivergents, aren’t responsible for our own reactions and behaviours — we certainly are, to the extent that they are under our control.
This is much larger than any individual, neurodivergent or not. It’s about a societal norm that says things like “if you’re getting picked on, just stop acting weird” instead of “stop being a jerk and picking on someone just because they’re different.”
I’m weird and proud of it, so what? I’m old now and have a lot fewer shits to give about what others think.
© Jillian Enright, Neurodiversity MB
Small self-promotion
A short clip of me talking about the social model of Rejection Sensitive Dysphoria (RSD) on NPR’s podcast, The Pulse (I was not paid for, nor do I receive any financial benefit from, my participation).
I discuss the social model of Rejection Sensitivity Dysphoria (RSD), ADHD, Autism, and neurodivergence around 23:30.
Related Articles
When you join medium, as a member you’ll have access to unlimited reads for only $5 per month. If you use my referral link, I’ll earn a small commission, and you’ll earn my undying gratitude.
If you’d prefer give a one-time tip, you can support my writing on Ko-Fi — also, it’s free to follow me on Facebook and LinkedIn!

References
Andrade, B. F., Waschbusch, D. A., Doucet, A., King, S., MacKinnon, M., McGrath, P. J., Stewart, S. H., & Corkum, P. (2012). Social Information Processing of Positive and Negative Hypothetical Events in Children With ADHD and Conduct Problems and Controls. Journal of Attention Disorders, 16(6), 491–504. https://doi.org/10.1177/1087054711401346
Barkley, Russell A. (2015). Attention-Deficit Hyperactivity Disorder: A Handbook for Diagnosis & Treatment. The Guilford Press.
Bong, S. H., Kim, K. M., Seol, K. H., Kim, J. W. (2021). Bullying perpetration and victimization in elementary school students diagnosed with attention-deficit/hyperactivity disorder. Asian Journal of Psychiatry, 62, 102729. https://doi.org/10.1016/j.ajp.2021.102729
Grygiel, P., Humenny, G., Rębisz, S., Bajcar, E., & Świtaj, P. (2018). Peer Rejection and Perceived Quality of Relations With Schoolmates Among Children With ADHD. Journal of Attention Disorders, 22(8), 738–751. https://doi.org/10.1177/1087054714563791
Hirsch, O., Chavanon, M., Riechmann, E., Christiansen, H. (2018). Emotional dysregulation is a primary symptom in adult Attention-Deficit/Hyperactivity Disorder (ADHD). Journal of Affective Disorders, 232, 41–47. https://doi.org/10.1016/j.jad.2018.02.007
Hoza, B. (2007). Peer Functioning in Children With ADHD, Journal of Pediatric Psychology, 32(6), 655–663. https://doi.org/10.1093/jpepsy/jsm024
Jellinek, M. (2010). Don’t Let ADHD Crush Children’s Self-Esteem. Clinical Psychiatry News. https://mdedge.com/psychiatry/article/23971/pediatrics/dont-let-adhd-crush-childrens-self-esteem
Jurgens, A. (2020). Neurodiversity in a neurotypical world. In Bertilsdotter Rosqvist, H., Chown, N., & Stenning, A. (Eds). Neurodiversity Studies: A new critical paradigm. Routledge.
Sobanski, E., Banaschewski, T., Asherson, P., Buitelaar, J., Chen, W., Franke, B…. Faraone, S.V., et al. (2010). Emotional lability in children and adolescents with attention deficit/hyperactivity disorder (ADHD): clinical correlates and familial prevalence. Journal of Child Psychology and Psychiatry, 51: 915–923. https://doi.org/10.1111/j.1469-7610.2010.02217
Walerius, D. M., Reyes, R. A., Rosen, P. J., & Factor, P. I. (2018). Functional Impairment Variability in Children With ADHD Due to Emotional Impulsivity. Journal of Attention Disorders, 22(8), 724–737. https://doi.org/10.1177/1087054714561859
Walker, N. (2021). Neuroqueer Heresies: Notes on the neurodiversity paradigm, Autistic empowerment, and postnormal possibilities. Autonomous Press.
Wiener, J., Mak, M. (2009). Peer victimization in children with Attention-Deficit/Hyperactivity Disorder. Psychology in the Schools, 46(2), 116–131. https://doi.org/10.1002/pits.20358




