
Are The “Brain Dead” Really Dead?
The Ethics of Brain Death & Organ Transplantation
Of the 106,000 people on the national organ transplant waiting list, only a small fraction will receive the potentially life-saving procedure. Medical professionals are constantly searching for new ways to treat those who experience organ failure and other chronic conditions.
There have been promising results in researching the use of manufactured and animal organs for human transplantation. However, the ways in which researchers can ethically experiment with and test these methods are limited.
Many believe that brain-dead individuals are the clear and simple solution to ethically conducting organ transplant experiments, and could perhaps eliminate the need for such experimentation in the future. Organ transplantation experiments on brain-dead individuals could save countless lives, but are they ethical?
How can we know the “brain dead” are actually dead and how can we be sure these experiments are truly consensual?
Defining Death
Most people in their everyday language define “death” as what happens after your last heartbeat. However, according to the Uniform Determination of Death Act (UDDA), there are two criteria for medical death. The first is quite recognizable: “irreversible cessation of circulatory and pulmonary functions.” Aka loss of function in the heart and lungs.
Yet 2.06% of deaths in the United States meet the second more contemporary criterion: Brain death. Now, death by neurological criteria has become a medical and legal standard accepted around the world.
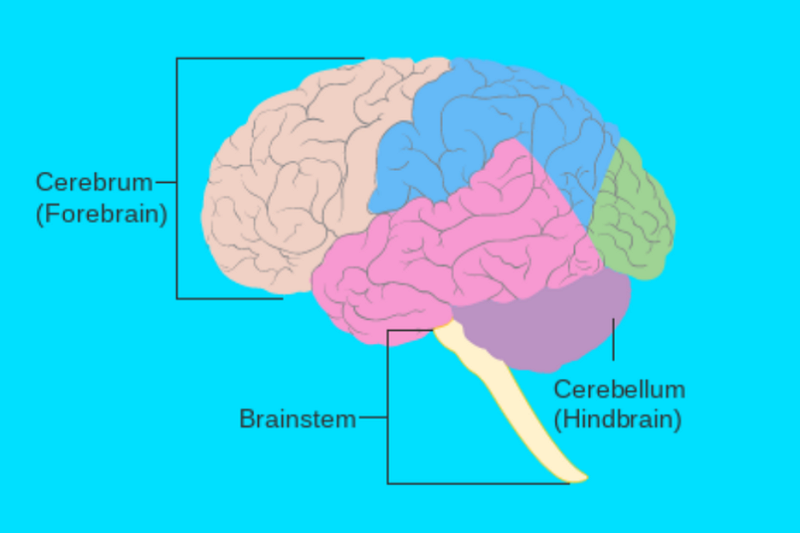
Brain death, as currently defined, occurs with irreversible cessation of all functions in the brain including the brain stem. In other words a total and irreparable failure of the entire brain and brain stem. that second part is important, a patient who has lost all major brain functions of all parts save for the brain stem would not meet this criterion for death.
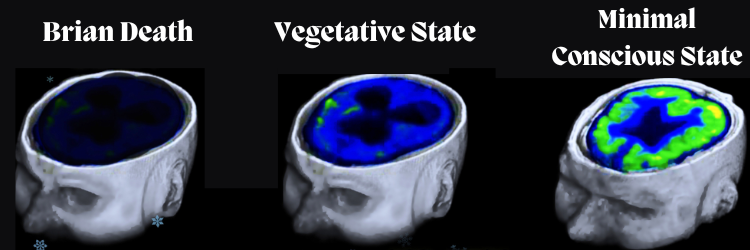
Patients who experience severe brain trauma may enter into an irreversible coma or a persistent vegetative state and rely on daily medical intervention to live. While it is rare, these conditions are technically reversible and thus do not meet the neurological standard for death. Because it is possible that these individuals could recover and possibly return to personhood, we cannot ethically consider them deceased.
History of Brain Death
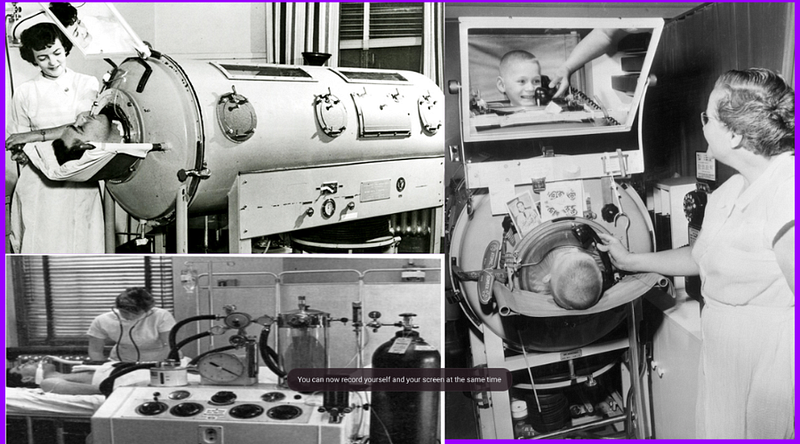
In the 1950s and 60s, the grayscale nightmare machines you see above (ventilators) were rapidly becoming available for widespread use. This caused a wave of changes in our perception of medical practices and norms. Nueriolgicaly impaired patients who would otherwise quickly die due to lack of respiratory function could not be kept alive artificially.
The ethical debate surrounding these practices and treatment of those then called “hopelessly unconscious” or in reversible comas, ensued almost immediately.
These new methods of life-sustaining intervention fed into the newly emerging field of human organ transplantation, in which the best success was found with organs that are oxygenated right up until the time of transplant. Artificially sustained patients on respirators could maintain oxygenated organs until the time of transplant, greatly increasing the likelihood of success.
In 1968, a Harvard Medical School committee published a set of guidelines to address brain death and irreversible comas. They contend that irreversible comas should be conceived of as a new form of death. In the years after its publishing, many states developed laws allowing physicians to declare the death of patients on ventilators by lack of brain function. Largely endorsing what came to be known as “The Harvard criteria.”
The brain death standard has been recently adopted by pro-choice proponents as a justification for early abortion. “Brain birth” posits that, just as the brain-dead individual is no longer living, the human fetus, before possessing a developed brain, is not yet living.
Ethical Considerations
As brain death has become more accepted and standardized experiments have become more common. The University of Alabama at Birmingham recently announced the first clinical-grade transplant of gene-edited pig kidneys into a brain-dead human. This is also the first-peer reviewed study to establish brain-dead individuals as viable clinical models.
Over 600,000 patients waiting for kidney transplants depend on dialysis to survive, 240 of which die every day. New research in genetic editing has allowed researchers to discover new ways to make animal organs compatible with the human immune system. The ability to successfully transplant animal organs could save and improve countless lives.
The controversy, in part, comes from the obvious medical analogies that can be drawn. Someone who cannot live without medical intervention, say a dialysis patient, certainly still has bodily autonomy and a right to life. So why are cases of brain death treated differently from other cases?

It is because the condition of brain death is irreversible, much like the first criteria, and though they can maintain their vital functions through technology, people who experience brain death no longer have the capacity or potential capacity for conscious experience. Philosophically they may be viewed as an empty vessels, organs without an owner. Much like one would not consider a heart pumping in a jar human life. The diseased, though their organs survive are considered to no longer have the moral value of a living person because their minds, their conscious identity, memories, arguable anything that makes them who they are has ceased to exist.
Many have accepted these standards due to the notion that moral value and individuality are not determined by our health or capabilities but rather, contained in the mind. This thinking can be reconciled with most modern worldviews.
Materialism: Our self is purely material and our conscious experience does not extend beyond the physical brain. Brain death is death.
Theism: Our spirit is manifested in our physical mind and in turn our material brain. The body is not the true or infinite self. Brain death is death.
In terms of ethics, the first issue would have to be achieving an accurate diagnosis. If we accept, as many have, that brain death is true death then the first step is to ensure that those who we treat as dead are actually under irreversible conditions rather than a persistent vegetative state or coma which can be argued to be a separate ethical issue, as these patients have the potential to recover and are not considered deceased.
Medical professionals have developed strict standards and new technology to recognize and diagnose brain death. Most cases are determined through high-tech scans or studies, but rather a physician will test the patient's reactions to outside stimuli such as bright light and whether the patient can breathe on their own. A diagnosis of brain death requires persistent coma, absence of brainstem reflexes, and lack of any ability to breathe independently.
It is crucial moving forward that terms and methods of diagnosis are clearly defined as a misdiagnosis could easily lead to unethical human experimentation on an unconscious individual.’
Now that we have a uniform and accepted standard for death, the next question is whether it is ethical to experiment on these patients in the field of organ transplantation. Cadavers have long been used for medical research, most ethnically when one's body is voluntarily donated. If there is an accurate diagnosis of brain death then there is no conceivable reason to ethically treat the individual differently than a cadaver or recently deceased person.
“Everybody, every human being has the obligation to contribute to this world.” — Edith Carter, Holocaust Survivor
Deontological ethics, world religions, and human culture, in general, cultivate empathy for human remains. Brain-dead patients should not be discarded or experimented on frivolously.
A deontological approach, in the case of organ transplantation research, would likely recognize a duty to improve the world as well as the autonomy of the deceased to determine the fate of their remains. Of course, this assessment is not uniform and approaches will differ depending on the deontological system to which one subscribes. However, outside of cultures with very strict funerary rights and rituals, it does not seem likely that there would be many objections to such experimentation, assuming the consent or surrogate consent of the individual.
Deontology- the study of the nature of duty and obligation.
Utilitarniasm- the doctrine that actions are right if they are useful or for the benefit of a majority.
Through utilitarian ethics, the solutions are much clearer. Human transplantation experiments have an immeasurable potential to improve and extend the lives of humans, greatly improving the opportunity for a positive experience and, through the principle of aggregation, greatly increasing the goodness of the world. Furthermore, in the case of the brain dead through this enlightened view, there is no harm caused in the pursuit of these experiments. Organ transplantation research and experimentation after brain death is a win-win for utilitarianism. In the broader sense, setting a precedent for research on the brain dead will reduce the need for living human and animal experiments, even further improving the utilitarian quality of the world.
Another such issue is whether experimentation on the brain dead is actually consensual. Many individuals have not made premortem decisions about how their remains should be treated and if their salvageable parts are available for research or donation. Since it is impossible to know postmortem wishes it is common to turn to those who knew the individual best and seek surrogate consent.
The ethics of making a decision for an individual who can no longer speak for themselves may still be up for debate, however, it is commonly accepted that those with degenerative neurological disorders, in comas or in persistent vegetative states will give power of attorney or the right to make a decision on their behalf to a family member or other beneficiary. The precedent for third-party medical decisions is there and arguably even easier to apply to those who are now classified as deceased through UDDA standards. In the event that medical professionals are unsure of an individual's postmortem wishes, it seems it is still ethical to seek the consent of the person’s family.

While there will always be issues, such as making the correct diagnoses, and what experiments themselves are ethical to conduct. It seems clear that we can apply the same ethics as cadavers and human remains to those who die by neurological standards. Experimentation on those who experience brain dead is a pragmatic and tangible route to improving the lives and health of American society. Further, it seems the practice occurring within the parameters defined by medical standards can be justified from a utilitarian as well as a deontological approach while not violating any intuitive standards of scientific research or differing worldviews.
TL;DR: Allowing and expanding research on brain-dead individuals, especially in the case of organ transplantation, is an ethical way to significantly improve medical technology and lead to a slew of health and societal benefits including a reduction in unethical or undesirable scientific research.


Follow -> ⭐ Facebook ⭐ Twitter ⭐ Vocal.Media





