
HEALTH AND SCIENCE
A Beginner’s Guide to Cancer and Current Thinking on How to Beat It
An overview of research on genetic and metabolic causes of cancer and strategies to prevent and treat ‘The Big C’
Cancer is a frightening disease. Much like Voldemort, people are often reluctant to even say its name, preferring to speak in euphemisms about ‘The Big C’ or ‘Jack the Dancer.’
When former US President Richard Nixon announced ‘the war on cancer’ in 1971, many hoped that cancer would soon be a thing of the past. Sadly, however, after more than 50 years, we have frustratingly little to show for our decades of research.
Our understanding and treatments have both made important strides. But successes are the exception, not the rule, and cancer death rates have not seriously improved in decades despite our best efforts.
If our conventional approach works well for particular cancers but fails to treat most types of cancer, what are we getting wrong? How can we improve? And how can we reduce our personal risk of getting cancer?
Today, we’ll cover what’s currently known about these questions.
1 – Outline
We’ll start with a quick overview of cancer and how people viewed it over time. We’ll explain how genetic mutations became enemy number one in the war on cancer, how the genetic-pharmaceutical approach to treating cancer became orthodoxy, and describe some success stories of this approach, such as Glivec (also written as Gleevec).
However, we’ll also briefly look at issues with the genetic-mutation theory of cancer, explain why the genetic-pharmaceutical approach to treatment has generally failed, and why this approach seems unlikely to succeed in the near future.
To finish, we’ll talk about a new wave of research looking at cancer from metabolic and evolutionary perspectives. This work is very exciting, as it offers novel ways to beat cancer and practical advice for reducing our risk of contracting the disease.
Let’s dive in.
2 — What is cancer?
Cancer is as old as multicellular life, and its history stretches back as far as we can see. For example, cancer has been found in dinosaur fossils from millions of years ago.
Despite some popular myths, like that sharks don’t get cancer, we also know that wherever you find multicellular life, you virtually always find cancer. Rare exceptions include oddballs like comb jellyfish and sea sponges.
{kind=link}
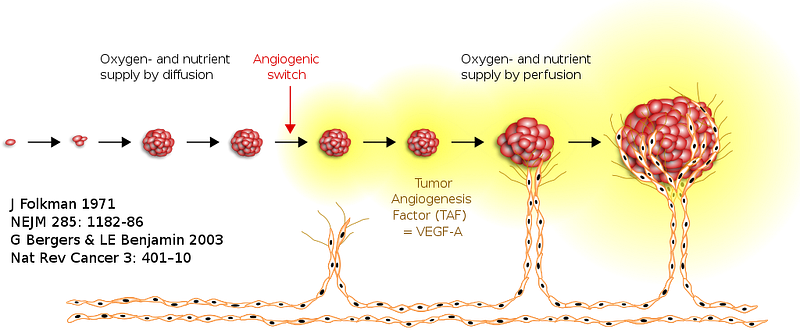
Cancer occurs when cells grow uncontrollably. If left unchecked, these rogue cells can proliferate by redirecting blood flow to themselves, pilfering resources and bodily real estate from their law-abiding neighbours. This is how tumours form.
A tumour is cancerous (‘malignant’) when it invades other tissues and organs of the body. By contrast, tumours are not considered cancerous (‘benign’) when they don’t invade neighbouring tissues and other organs.
This doesn’t apply to all cancers, such as cancers of the blood (e.g., leukemias), which usually don’t form tumours.
When we talk about the dangers of ‘cancer’, and ways to treat it, we’re mostly talking about the malignant kind. But a lot of what we’ll cover applies to both benign and malignant cancer.
3 — How did we understand cancer over time?
Until recently, we knew remarkably little about cancer. Part of the problem was that cancer can take many forms.
Dissection of deceased human bodies was also taboo for centuries, and we learned very slowly, particularly when disease and death were seen as divine judgment.
Another mystery was that cancer seemed to be associated with many environmental factors, most of which didn’t have anything obvious in common.
For example, people noticed that exposure to lots of dirty air increased the risk of various cancers, such as the so-called ‘chimney boys’ of 18th century Europe. Today, we know that many air-borne materials can cause cancer (e.g., pollution, asbestos, smoking).
It was also known that infections could increase our risk of getting certain cancers, like cervical cancer in women. In the age of germ theory, we have since identified human papillomavirus (HPV) as the culprit.
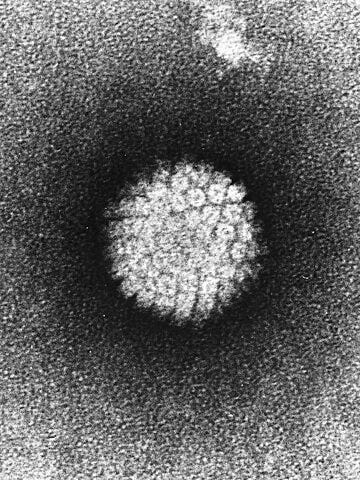
_EM.jpg){kind=link}
Despite their confusion, people were clearly on the right track. But the question remained: how could such different causes lead to the same disease?
4 — The genetic-mutation theory of cancer
Mendelian genetics and essentialism in Western psychology
Gregor Mendel’s work on biological inheritance in pea plants was discovered by mainstream science in 1900. This laid the foundation for the new discipline of genetics, which really took off after the molecular structure of DNA was discovered in the 1950s.
Genes appealed to the essentialism of Western psychology, and they soon took center stage in conventional thinking about life, human nature, health, and disease.
Famous and influential examples of this include The Selfish Gene by Richard Dawkins and the books Sociobiology: The New Synthesis and On Human Nature by the late Harvard evolutionary biologist Ed Wilson.
This work and popular writing also created the field of sociobiology, which popularised the idea that we are our genes (aka ‘genetic reductionism/determinism’).
Genetic mutations and cancer
During the 1950s and 1960s, people applied this logic to the causes of cancer, and soon found their prime suspect: genetic mutations.
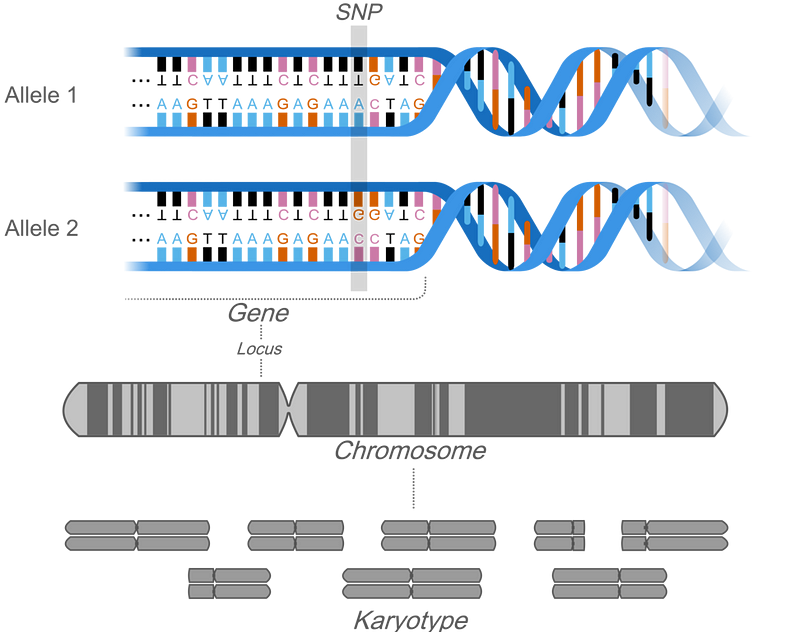
{kind=link}
This was a masterstroke, as we now know that different cancer risk factors, from viruses and pollution to radiation and sunlight, can all cause genetic mutations.
Researchers also found genetic mutations that made perfect sense, given that cancer is a disease of uncontrolled cell growth.
For example, many cancer cells have mutations in genes that tell cells not to grow (‘oncogenes’), and in genes that command rogue and/or damaged cells to commit suicide (‘tumour suppressor genes’). These mutations prevent the genes from doing their work, which allows cancers to grow.
The genetic-pharmaceutical approach to cancer
Based on these discoveries, the strategy to fight cancer seemed obvious: identify mutated genes and find drugs to correct the problem. (Of course, where possible, surgery is another valuable option.)
The poster child of this approach is Glivec (or Gleevec), which is effective at treating leukemia. As we’d expect, it works by inhibiting cell growth and instructing cancerous cells to commit suicide (‘apoptosis’).
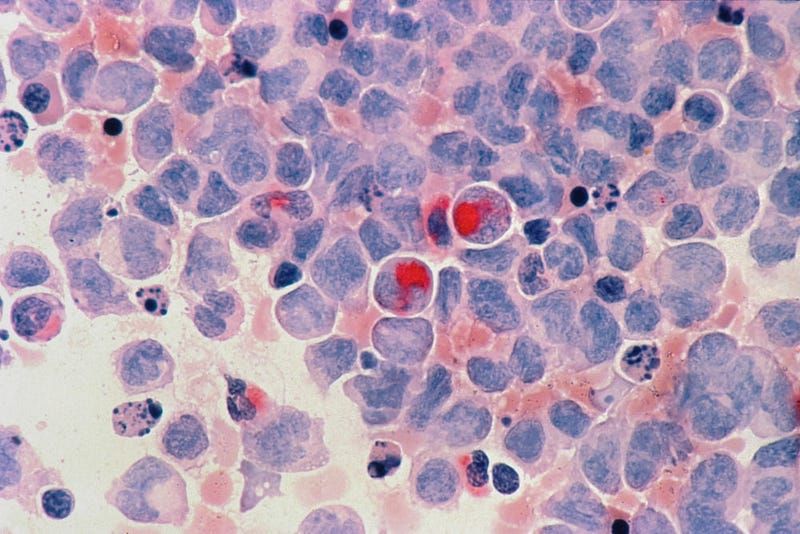
5 — Issues with the genetic-mutation theory of cancer
Sadly, however, Glivec may be the high-water mark for the genetic-pharmaceutical approach to cancer, as similar success has not been achieved for other cancers.
What’s more, a body of contrary evidence has steadily grown too large to ignore.
Some genetic mutations were mistakenly linked to cancer
For example, studies found that some genetic mutations implicated in cancer were also present in perfectly healthy cells.
Many researchers seem to have been overly keen to find cancerous genetic mutations, and succumbed to confirmation bias.
Genetic damage in cancer cells is often weirder than theory predicts
As geneticist Kat Arney details in her book Rebel Cell, the genes of many cancer cells also have unexpected types of damage and behaviour.
Unlike the handful of important genetic mutations predicted by theory, some cancers are littered with genetic carnage, as whole chromosomes can be deformed.
For reasons that remain unclear, entire chromosomes may also copy themselves too many times.
These findings are completely alien to the genetic mutation theory of cancer, suggesting that mutated genes are not the whole story.
Cancer cells are usually subdued when surrounded by healthy cells
In his recent book Transformer, evolutionary biochemist and cancer researcher Nick Lane points out another quirk of cancer that doesn’t conform to theory: cancer cells usually stop behaving cancerously when they’re transplanted into healthy tissue.
If cancer was purely about cells with mutated genes, this is not what you’d expect to see. This indicates that the cellular microenvironment also influences cancer risk and that cancer is more than simply rogue cells with an unlucky combination of genetic mutations.
(In fairness, Kat Arney also makes this point. But I needed to introduce Nick Lane, and it was convenient to leave her out. Sorry, Kat.)
Cancer death rates haven’t improved much since the 1950s
Both Kat Arney and Nick Lane also highlight how improvements in cancer death rates have been quite modest.

{kind=link}
Granted, we now take longer to die from cancer. But we’re just as likely to die as we were in the 1950s, despite investing decades of research and mountains of resources.
This is especially true for some of our most lethal cancers. For example, there are currently no known effective treatments for the most common type of brain tumour, glioblastoma. Not even surgery, which usually leaves residual cancer cells that seed the next wave of tumours.
Glioblastomas grow and spread quickly, though usually only within the brain and/or spine. Unfortunately, they seem to always contain a subset of hyper-aggressive cells that defy all available types of therapy (e.g., radiological, chemical, immunological). This essentially guarantees the eventual recurrence of terminal brain tumours.
Glioblastoma can kill within 6 months after diagnosis. Currently, our best treatments only increase average life expectancy by 14.6 months.
For glioblastomas, and cancers in general, much of the issue boils down to a stubborn weakness in our current approach to cancer: drug resistance. More on this in a moment.
6 — New ways to understand and treat cancer
Due to these shortcomings in our standard theory and treatments for cancer, researchers sought novel ways to approach the problem. Currently, two promising areas of research involve metabolism and evolution.
Cancer and metabolism
Cancer metabolism has become an exciting area of research in recent years. But the role of metabolism in cancer has fascinated scientists ever since the 1920s.
{kind=link}
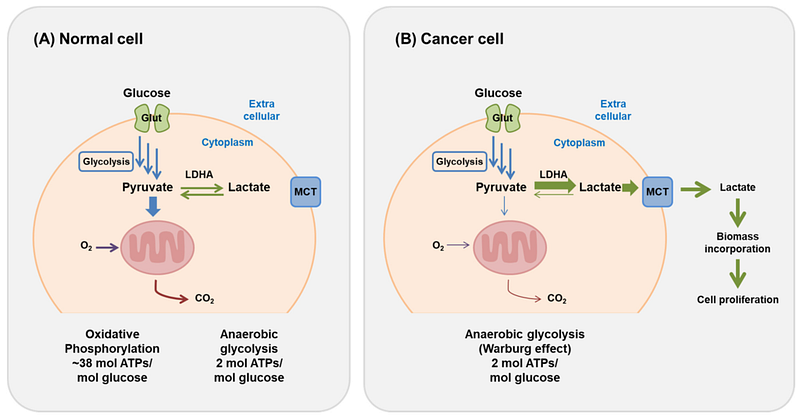
It began when Otto Warburg (1883–1970) showed that cancer cells often prefer to ferment sugars for energy rather than follow a conventional oxygen-dependent (‘aerobic’) form of metabolism. This occurs even in the presence of oxygen and is known as the Warburg effect.
The reasons for this have been much debated, and Warburg himself had some fairly zany ideas that were based more on ego and pride than science.
However studies in recent years have cast new light on cancer metabolism, with many encouraging discoveries. Even better, this research suggests some simple and practical ways to lower our risk of cancer.
The key finding is that cellular metabolism can work in a number of ways. This will be news to the majority of people who only learned about the conventional pattern of metabolic flux, discovered by Hans Krebs in 1937: the Krebs cycle (aka citric acid cycle).

{kind=link}
Importantly, Nick Lane explains that some patterns of metabolic flux push our cells in a cancerous direction, increasing our risk of getting the disease.
This can occur in a variety of ways. For example, if a cell is tricked into thinking it’s starved of oxygen, it will resort to fermenting sugars for energy, which increases the chance that the cell will become cancerous.
This is another instance of the Warburg effect and can be caused by mutations in genes for key metabolic enzymes. The Warburg effect can also be driven by other factors that lower our cellular oxygen supply (e.g., bacterial infections), and then locked in place by an unlucky combination of genetic mutations.
This synthesis between genetic and metabolic factors is a promising step, as it helps to reconcile how genetic mutations and the cellular microenvironment both seem to contribute to cancer.
Lifestyle factors and staying healthy
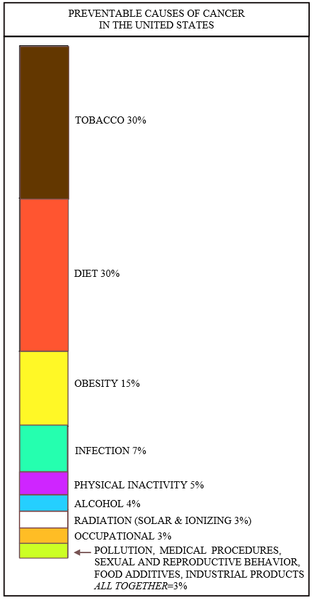
This also sheds light on how certain lifestyle factors are linked to cancer. For example, everyone is aware that smoking increases our risk of cancer, as does obesity/poor diet, pollution, and ultraviolet light.
{kind=link}
But a more surprising finding is that sedentary lifestyles increase our risk of cancer. People like Nick Lane suggest that this may also explain why age is the number one risk factor for cancer, as we become more sedentary as we get older.
The exact reasons for this are now the subject of intense study. But current thinking is that sedentary lifestyles disturb our preferred form of metabolism: the Krebs cycle.
Like the Warburg effect, this forces our cells to adopt different patterns of metabolic flux, which can increase our risk of cancer. And if we’re unlucky, genetic mutations can then make this cancer-prone metabolic shift permanent.

Fortunately, there’s a simple solution: stay physically active for as long as possible.
Using evolutionary thinking to beat drug-resistant cancer
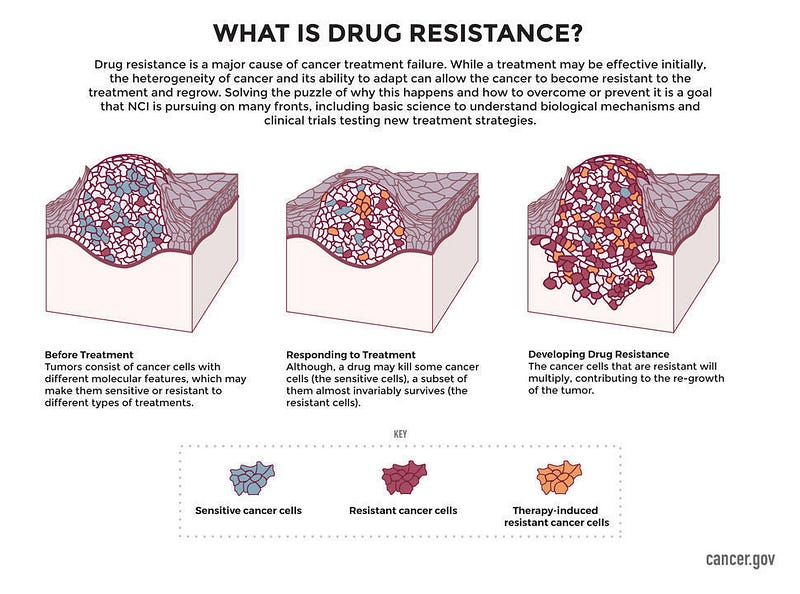
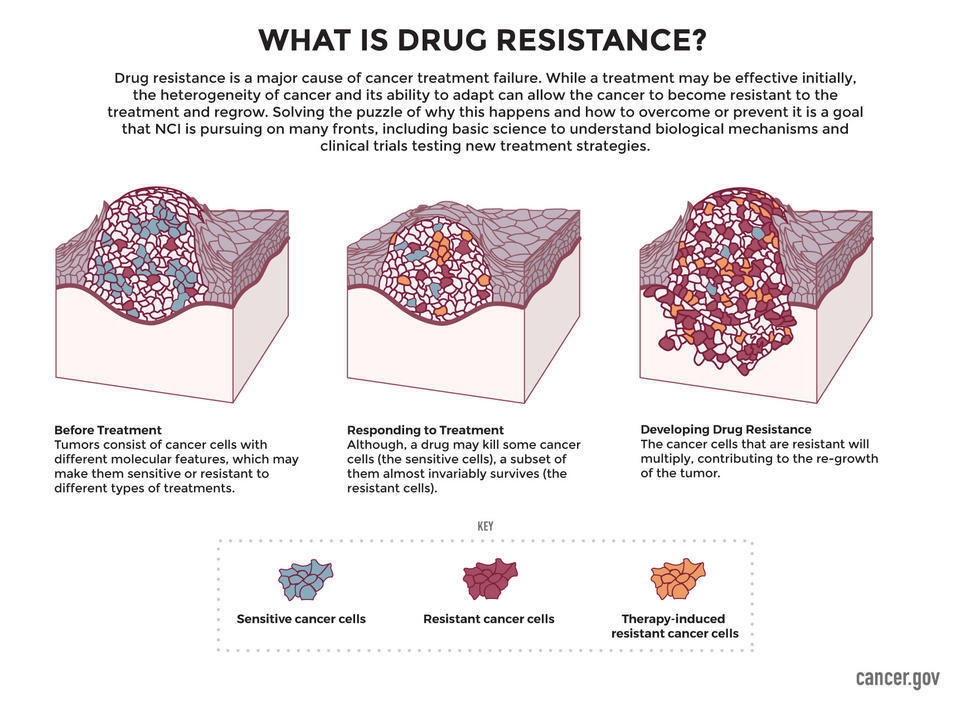
As we alluded to, drug resistance is one of the main hurdles for the genetic-pharmaceutical approach to cancer.
No matter what drug we try, there always seems to be a minority of cancer cells that are, or soon become, resistant to the drug. This is classic Darwinian variation and selection operating at the cellular level.
Cancers may appear to go away as the majority of drug-affected cells are killed. But the drug-resistant minority continues to grow until the cancer is back, and now it’s immune to the drug you used last time. Needless to say, this isn’t the win we’re searching for.
People tried to beat this problem using cocktails of drugs, hoping that no cancer cell would develop resistance to multiple drugs at once. But this tactic hasn’t worked so far, as cancer cells are vexingly adaptable.
{kind=link}
To escape this Darwinian trap, researchers are now using evolutionary thinking to turn cancer cells against each other.
They apply the treatment and wait for the tumour to go into remission. This weakens all cancer cells except the drug-resistant minority. They then pause the treatment and let the drug-affected and drug-resistant cancer cells fight amongst themselves for resources and territory.
The genius of this approach is that it turns the Darwinian process from a weakness into a strength – using cellular evolution as a tool, rather than as an obstacle to overcome.
Studies indicate that this approach, known as adaptive therapy, can significantly improve length and quality of life. It isn’t a cure, but adaptive therapy may allow us to safely manage cancer for extended periods.
This can buy precious time in the twilight of our lives and allow us to live long enough to die on our own terms.

For these reasons, many find adaptive therapy more attractive than long, expensive, and unpleasant cancer treatments, especially since these therapies will most likely lead to drug-resistant cancer sooner or later.
Conclusions and takeaways
Discovering genes and their role in cancer were landmark achievements. Unfortunately, however, this wasn’t enough to win the war on cancer.
Genetic mutations clearly play a role in cancer, and successes like Glivec are definitely worth celebrating. However, an overly gene-centric perspective blinded us to the limits of this approach and led us to neglect important lifestyle and metabolic factors.
While nothing is failsafe, our best evidence suggests that staying physically active, not smoking, and maintaining a healthy weight will significantly lower our risk of cancer.
Drug resistance is a cruel phenomenon, and one which the genetic-pharmaceutical approach seems unlikely to overcome, based on our efforts so far. But treatments that take evolutionary dynamics into account, like adaptive therapy, offer new ways to thwart cancer.
True, this isn’t the silver bullet we’ve sought. But if we can outrun cancer until we die at a ripe old age rather than defeat cancer on the battlefield of medicine, the results aren’t very different from a cure. After decades of dead ends and blind alleys, at least it’s nice to have new reasons for hope.
Good health, happy holidays, and thanks for reading!