
Neurodiversity | Mental Health
My ADHD Was Misdiagnosed as a Personality Disorder
Why this so often happens to people who are already marginalized

In January of 2010, I was labelled “Borderline”.
After two years of battling serious health issues, I had finally received a diagnosis of Celiac disease. This was good news. After many specialist appointments, we finally had an answer, and the treatment was strict adherence to a gluten-free diet. Maybe not super easy at first, but certainly not the worst of the possibilities we had been exploring.
Once I was no longer able to focus all my attention and mental energy on various medical appointments and diagnostic tests, the anxiety and emotional weight of the previous two years finally came crashing down on me. How ironic: my physical health was finally improving while my mental health began its steep decline.
The previous two years had been horrible.
I had to stop attending my University courses because I was too unwell. I was forced to demote myself at work because I couldn’t keep up with the demand. I had my driver’s license suspended for one year due to the seizures, removing some degree of freedom I had enjoyed for a short time. I had purchased my first car in 2007, only to put it up on proverbial blocks in 2008.
I had been too sick, and was spending too much time in doctors’ offices, to process all of this while it was happening. When I finally stopped moving forward, the pain caught up with me. I became severely depressed, spending entire days in bed. I often wouldn’t get up until my (newlywed) husband arrived home from work, and many times that was simply to move to the couch with a glass of wine in hand.
It gets worse before it gets better.
Finally, with the loving support of my husband, I sought help. I received a referral and eventually met an amazing psychiatrist. She was very smart and to the point. She called me on my B.S. and didn’t mince her words. Her approach worked very well for me. Sadly, only a few months after meeting Dr. M, she had to move out of the province. I was referred to another psychiatrist who was smart enough, he just didn’t listen.
I was bloody smart too, if I may say so, although mental illness was clouding my judgement. I had two related degrees, the second of which was in psychology. I was no expert, but I wasn’t completely clueless either. This doctor tried to mansplain my own mental health issues to me without actually hearing what I was communicating about my experience and my symptoms.
This doctor tried to mansplain my own mental health issues to me without actually hearing what I was communicating about my own experience and symptoms.
With relatively little information, the new psychiatrist diagnosed me with Borderline Personality Disorder (BPD) and prescribed me antidepressants and cognitive-behaviourally oriented dialectical behavioural therapy (DBT).
What does this have to do with misogyny?
While I don’t know what that particular doctor’s thought process was (and this was over a decade ago), this experience is unfortunately very common even today, especially for marginalized genders. This includes CIS-women, trans, and non-binary people.
Clinicians often (wrongly) operate on the assumption that anyone considered female simply can’t have ADHD. It’s stereotypically considered a “boy’s” disorder.
When people talk about male and female presentations of neurodiversity, they usually mean internalizing versus externalizing symptoms.
Traditional “female” presentations refer to internalizing symptoms, for those with ADHD, that would include symptoms such as inattentiveness and anxiety. These symptoms are often overlooked when considering neurodiversity, and a female-presenting patient would more likely be labelled with an anxiety or personality disorder.
Traditional “male” presentations include externalizing symptoms such as impulsivity and aggression, which are more disruptive to others, and as a result are more often brought to the attention of clinicians. These externalizing symptoms are also more in line with the stereotypical view of ADHD, making it easier for male-presenting patients to receive a diagnosis.
In contrast, BPD is often considered a mental illness primarily impacting young women. Doctors hear of women making impulsive decisions, feeling anxious and emotionally dysregulated, and label them “borderline”. They hear the same symptoms in males and are much more likely to consider ADHD.
A Modern View
More recent studies have illuminated the gender bias in diagnosing personality disorders. For example, Busch and colleagues (2016) found minimal gender differences in Borderline Personality Disorder severity, and Skodol & Bender (2003) found that the differential gender prevalence of BPD in clinical settings appears to be largely a function of sampling bias.
In fairness, there are a lot of overlapping symptoms between BPD and ADHD, as described in a 2014 article in the Journal of Borderline Personality Disorder and Emotion Dysregulation (Matthies & Philipsen, 2014).
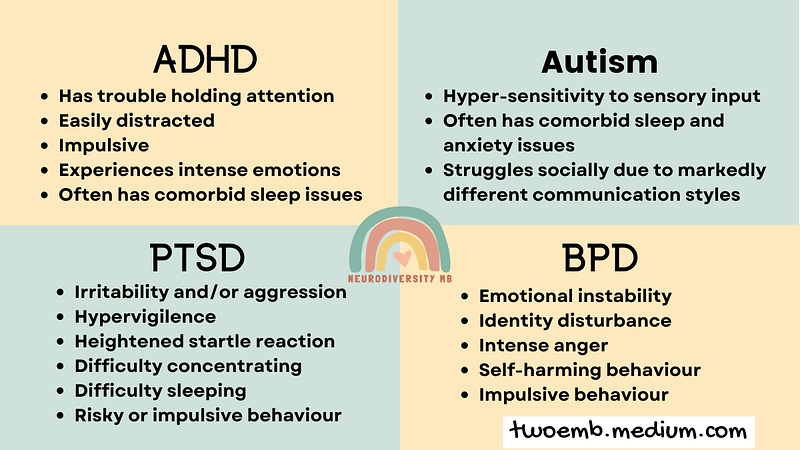
Research earlier this year identified significant similarities in emotional dysregulation and emotional intensity in both BPD and ADHD. Moukhtarian et al. (2021) concluded:
“…the presence or severity of emotional dysregulation should not be used in clinical practice to distinguish between the two disorders.”
More Missed Opportunities
Back in 2010, I was also finishing up my second degree and had a GPA of 3.7, despite having been sick for the better part of 2 years. It is often assumed that people with ADHD will have low grades and messy houses. For trained professionals, some sure oversimplify neurodevelopment and diagnosis.
Unfortunately, the DSM-V actually misses the most significantly impactful aspects of ADHD; the most glaring oversight being the lack of emotional dysregulation as a key symptom.
Dr. Russell Barkley, one of the world’s leading experts on ADHD, has been lecturing and writing about this life-impacting component of ADHD for many years (Barkley, 2015).
As it turns out…
I was actually quite lucky with this misdiagnosis because previous attempts to treat my anxiety and depression with Selective Serotonin Reuptake Inhibitors (SSRIs) had been unsuccessful, so the doctor prescribed a Selective Norepinephrine Reuptake Inhibitor (SNRI) instead.
Little did I know that SNRIs are often prescribed to patients with ADHD who do not tolerate stimulants well, commonly because of comorbid anxiety, which stimulants can make worse. SNRIs are also used as an adjunct with stimulants, called combination therapy, to treat patients for whom stimulants alone are not entirely effective (Budur et al., 2005).
It also turns out that DBT was helpful for my anxiety, as my anxiety was exacerbated by ( — or perhaps the anxiety caused) cognitive distortions. In essence, cognitive-behaviourally oriented DBT helps patients challenge distorted thoughts in order to break the cycle that feeds into anxiety.
DBT also teaches mindfulness, distress tolerance, and emotional regulation skills (Linehan, 2014) — skills that many people with ADHD, and really anyone, would benefit from.
Unfortunately, being misdiagnosed leads to inappropriate (or inadequate) treatment. So things got better, but not better better.
Fast forward…
A couple of years later, my husband and I had our son. He is one amazing dude. He is also a very intense kiddo.
When our son started school, we were told he was incredibly bright, but impulsive, and he struggled with anxiety and emotional regulation.
In 2018, he was assessed as being cognitively gifted, as well as diagnosed with ADHD, meaning he is twice-exceptional (or 2e). As I elaborated on in a previous blog post, “And Then There Were 2(e)…”, I was given the same diagnosis just seven months later, at the age of 36.
Vindication and Validation
Having studied ADHD in super-hyper-focus mode for the past three years, I can confidently say that I finally received the correct diagnosis. My ADHD has been effectively treated with medication, exercise, and other compensatory strategies, for a year and a half (19 months as of the end of May, but who’s counting?).
The right diagnosis and treatment can make all the difference. My quality of life has vastly improved and I’ve met some amazing neurodiverse friends and cohorts along my journey.
One of the best side-effects of my ADHD treatment is improved self-worth and self-acceptance. This is not only important for me, but for my son as well. He sees a Mom, who is much like him, managing her symptoms and accepting her differently-wired brain with all its quirks.
We often tease each other and laugh at ourselves for our forgetfulness and distractibility. We normalize the fact that there are many different types of brains in this world, and although ours come with some struggles, they also offer us strengths.
One of the best side-effects of my ADHD treatment is improved self-worth and self-acceptance.
© Jillian Enright, Neurodiversity MB
Related Stories
When you join medium, as a member you’ll have access to unlimited reads for only $5 per month. If you use my referral link, I’ll earn a small commission, and you’ll earn my undying gratitude.
If you’d prefer give a one-time tip, you can support my writing on Ko-Fi — also, it’s free to follow me on Facebook!
References
Barkley, R. A. (2015). Emotional dysregulation is a core component of ADHD. In R. A. Barkley (Ed.), Attention-deficit hyperactivity disorder: A handbook for diagnosis and treatment (p. 81–115). The Guilford Press.
Budur, K., Mathews, M., Adetunji, B., Mathews, M., & Mahmud, J. (2005). Non-stimulant treatment for attention deficit hyperactivity disorder. Psychiatry, 2(7), 44–48. https://ncbi.nlm.nih.gov/pmc/articles/PMC3000197
Busch, A. J., Balsis, S., Morey, L. C., & Oltmanns, T. F. (2016). Gender Differences in Borderline Personality Disorder Features in an Epidemiological Sample of Adults Age 55–64: Self Versus Informant Report. Journal of personality disorders, 30(3), 419–432. https://doi.org/10.1521/pedi_2015_29_202
Linehan, Marsha, M. (2014). DBT Skills Training Manual (2nd Edition). The Guilford Press.
Matthies, S. D., & Philipsen, A. (2014). Common ground in Attention Deficit Hyperactivity Disorder (ADHD) and Borderline Personality Disorder (BPD)-review of recent findings. Borderline personality disorder and emotion dysregulation, 1, 3. https://doi.org/10.1186/2051-6673-1-3
Moukhtarian, T.R., Reinhard, I., Moran, P. et al. (2021). Comparable emotional dynamics in women with ADHD and borderline personality disorder. Borderline Personality Disorder and Emotional Dysregulation, 8, 6. https://doi.org/10.1186/s40479-021-00144-y
Skodol, A.E., Bender, D.S. (2003). Why Are Women Diagnosed Borderline More Than Men?. Psychiatric Quarterly 74, 349–360. https://doi.org/10.1023/A:1026087410516




