
{kind=link}
CLUSTER B PERSONALITY DISORDERS
Brain Mapping: How I Got Diagnosed with Antisocial Personality Disorder
The diagnostic process for personality disorders

When I first suspected I might have mental health issues, I was unwilling to get help. It took me over 6 months of reading around and trying to understand what was going on before I decided to see a psychiatrist. The first time I became certain I had a personality disorder was when I read Malignant Self-love: Narcissism Revisited by Sam Vaknin.
There are a lot of common features in personality disorders, so even though the book mostly focused on Narcissistic Personality Disorder, it was very relatable. A friend also suggested I might have ADHD because he was a Special Educational Needs Teaching Assistant and had experience with students with it. First I was assessed for ADHD and diagnosed as combined type. Later I started going to therapy for early childhood trauma and attachment issues.
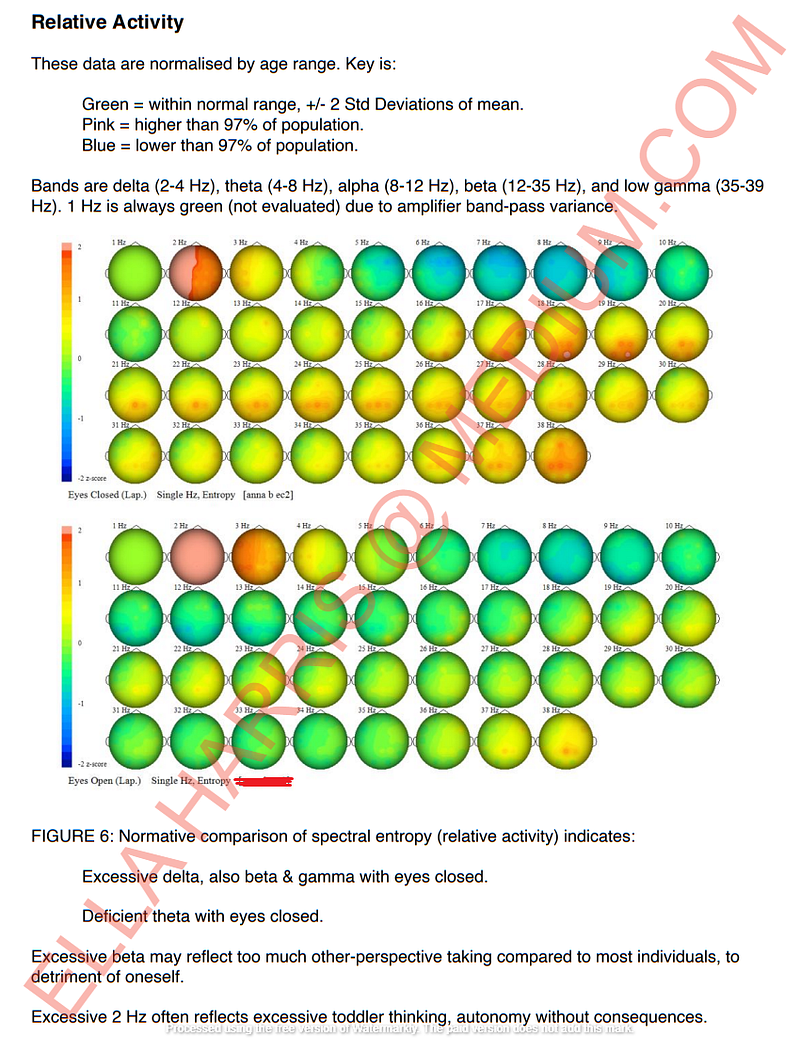
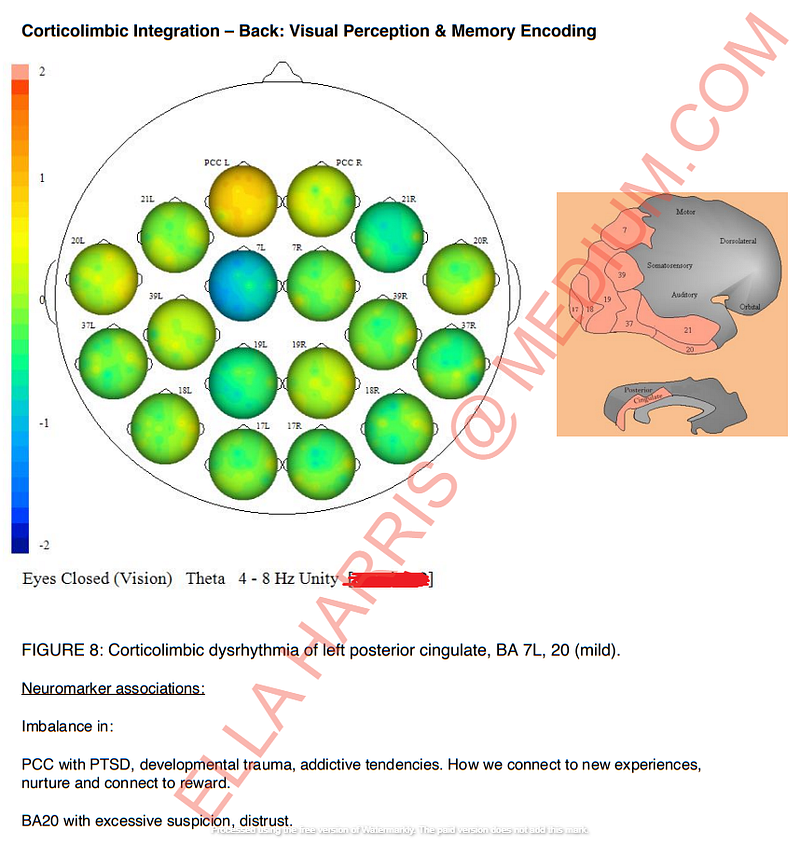
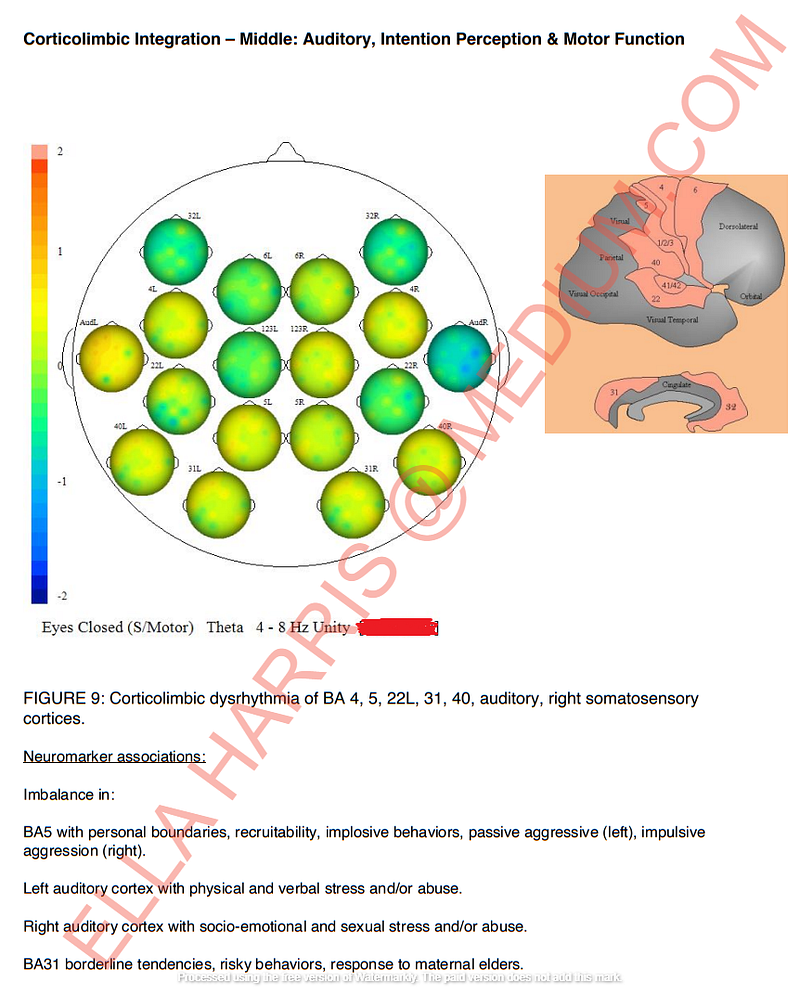
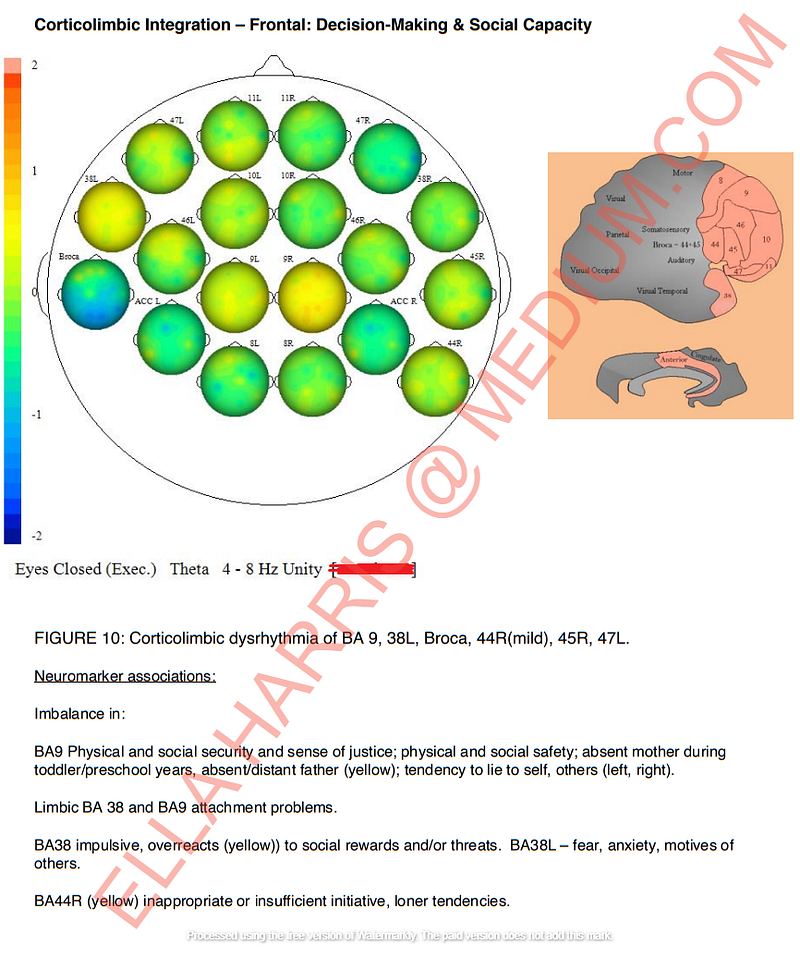
I decided to get assessed for personality disorders a year after that. I was looking into neurofeedback therapy for ADHD as medication was not effective in my case and my impulsivity was becoming problematic. I decided to get QEEG brain mapping done to begin with, which shows neuromarker associations with personality traits.
Shortly after the brain mapping, I saw a psychologist for an assessment of personality disorders. I took PAI (Personality Assessment Inventory) alongside a few other tests. Below are screenshots from the brain mapping and parts of the report from the psychologist:
Ms ‘…’’s clinical profile is marked by significant elevations across several scales, indicating a broad range of clinical features and increasing the possibility of multiple diagnoses. Profile patterns of this type are usually associated with marked distress and severe impairment in functioning. The configuration of the clinical scales suggests a person with a history of acting-out behaviour, most notably in the area of substance abuse but probably involving other behaviours as well. Her impulsivity and drug use have likely led to severe impairment in her ability to maintain social role expectations, and her recklessness may have alienated people who were once close to her. Generally impulsive and thrill-seeking, her use of drugs may further impair her judgment. Her interpersonal relationships are likely to be volatile and short-lived; even those relationships that have been maintained will have suffered some strain.
Ms ‘…’ indicates that her use of drugs has had many negative consequences on her life at a level that is above average even for individuals in specialized treatment for drug problems. Such a pattern indicates that her use of drugs has had numerous ill effects on her functioning. Problems associated with drug abuse are probably found across several life areas, including strained interpersonal relationships, legal difficulties, vocational failures, financial hardship, and/or possible medical complications resulting from prolonged drug use. She reports having little ability to control the effect that drugs are having on her life. With this level of problems, it is increasingly likely that she is drug dependent and withdrawal symptoms may be a part of the present clinical picture. The withdrawal syndrome will vary according to the substance of choice, but such syndromes can include many psychopathological phenomena such as concentration problems, anxiety, and depression.
She describes a personality style with numerous antisocial character features typically associated with prominent features of Antisocial Personality Disorder. Ms ‘…’ reported that relationships with others often failed due to frequent interpersonal conflict. While she may describe feelings of guilt over past transgressions, this may be short-lived. Her behaviour may be perceived as being reckless; she could be expected to entertain risks that are potentially dangerous to herself and to those around her.
Ms ‘…’ is probably quite impulsive and unusually energetic, it appears that her clinical picture is characterized primarily by heightened energy levels and irritability. She is likely to have an activity level that is perceptibly high to most observers. She is probably involved in these activities in an over-committed and disorganized manner, and she may experience her thought processes as being accelerated. Her relationships with others are probably under stress due to her frustration with the inability or unwillingness of those around her to keep up with her plans and possibly unrealistic expectations. At its extreme, this irritability may result in accusations that significant others are attempting to thwart her plans for success and achievement. However, grandiose thoughts and plans do not appear to be a strong feature of the clinical picture at this time.
Ms ‘…’ describes a number of problematic personality traits. Her responses suggest that a major problem for her involves her impulsiveness. This impulsivity seems to make her prone to behaviours likely to be self-harmful or self-destructive, such as those involving spending, sex, and/or substance abuse.
Ms ‘…’’s self-description indicates significant suspiciousness and hostility in her relations with others. She is likely to be a hypervigilant individual who often questions and doubts the motives of those around her. Although she may not describe herself as unduly suspicious, others may view her as very sensitive and easily insulted in her interactions. As a result, working relationships with others are likely to be strained and may require a degree of support and assistance in order to succeed.
According to Ms ‘…’’s self-report, she describes NO significant problems in the following areas: unusual thoughts or peculiar experiences; unhappiness and depression; marked anxiety; problematic behaviours used to manage anxiety; difficulties with health or physical functioning.
Environmental Factors
Ms ‘…’’s interpersonal style seems best characterized as remote and inward-focused. She is not likely to be very interested or invested in social relationships, and she may not equally contribute. She is probably sceptical of close relationships, preferring to engage in relationships that are within her control. She may avoid commitment in close relationships if possible.
In considering the social environment of the respondent with respect to perceived stressors and the availability of social supports with which to deal with these stressors, her responses indicate that she believes that her social relationships offer her little support; family relationships may be somewhat distant or ridden with conflict, and friends may not be available when needed. These relationship issues appear to be a current source of stress for her. Interventions directed at any problematic relationships (such as those involving family or marital problems) may be of use in alleviating a major source of situational pressures.
The self-concept of Ms ‘…’ appears to involve a generally positive self-evaluation. She is generally a confident, resilient, and optimistic person, although her self-esteem may be reactive to changes in her current circumstances. During times of stress, the respondent may inwardly be troubled by more self-doubt and misgivings about her adequacy than is readily apparent to others. Reactive changes in self-esteem may be accompanied by uncertainty about goals, values, and important life decisions.
Validity of Test Results
The degree to which response styles may have affected or distorted the report of symptomatology on the inventory is also assessed. Certain of these indicators fall outside of the normal range, suggesting that the respondent may not have answered in a completely forthright manner; the nature of her responses might lead the evaluator to form a somewhat inaccurate impression of the client based upon the style of responding described below. With respect to positive impression management, the client’s pattern of responses contains a number of subtle indications that positive impression management may be an area of concern. In attempting to make a good impression, she appears hesitant to admit to any negative consequences that might be associated with her actions or behaviour. This may lead to a tendency to minimize problems, particularly the impact or disruptive effects that any such problems have had upon her life and the lives of others. Individuals with this defensive style may tend to downplay disruptions in areas that close associates view as problematic. This level of defensiveness may not necessarily impair the interpretability of the test findings, but it does raise the possibility of distortion of the profile. The interpretive hypotheses in this report should be reviewed with these tendencies in mind because it is possible that the following interpretation underrepresents the extent and degree of any noteworthy findings. Particular attention should be paid to the possibility of denial of problems with drinking or drug use, as the respondent described certain personality characteristics that are often associated with involvement with alcohol or drugs. Given the impression management features noted above, she may be hesitant to disclose information about the extent of her use or the impairment that arises from such problems.
With respect to negative impression management, there is no evidence to suggest that the respondent was motivated to portray herself in a more negative or pathological light than the clinical picture would warrant.
Diagnosis
- Other (or unknown) substance use disorder, moderate
- Antisocial personality disorder
- Bipolar I disorder, current or most recent episode manic, unspecified
I’m sharing this because I want people to understand Antisocial Personality Disorder. There are a lot of myths surrounding psychopathy and people don’t quite understand what it means or immediately think of emotionless predators who are out to harm people. Personally, I prefer to think of personality disorders as disorders of attachment. I also don’t believe people without emotions exist but rather some people experience shallow affect, which means they are emotionally shallow and do not experience them as strongly. The video below is a good description of ASPD:
Here are the other articles I’ve written on Antisocial Personality Disorder:
If you enjoyed this post and would like to read more, you can subscribe here — https://medium.com/subscribe/@ella_harris to get an email whenever I publish a story. You can also buy me ☕ via — https://ko-fi.com/ella_harris
This post contains affiliate links. If you use these links to buy something I will earn a commission. Thanks.