
Why It’s So Unusual: Vaccine-Induced Blood Clots and Low Platelets
Making sense of the information on vaccine-induced thrombotic thrombocytopenia (VITT) out there to see what this is all about.
Unfortunately, the Oxford/AstraZeneca (Ox/AZ) and Johnson & Johnson (J&J) vaccines for Covid-19 have caused — or at least with high certainty of causing —a few cases of severe and fatal blood clots for every million doses of vaccine injected. Although this rate is minuscule — bearing possible underreporting in mind — one unwanted death is always one too many. And deaths with unclear causes need to be examined to prevent more of the same.
That said, let’s see what the vaccine-induced blood clots (accompanied by low platelet levels) — that make everyone anxious and worried — are all about. And what this means for you and the pandemic.
The numbers on vaccine-induced thrombotic thrombocytopenia (VITT)
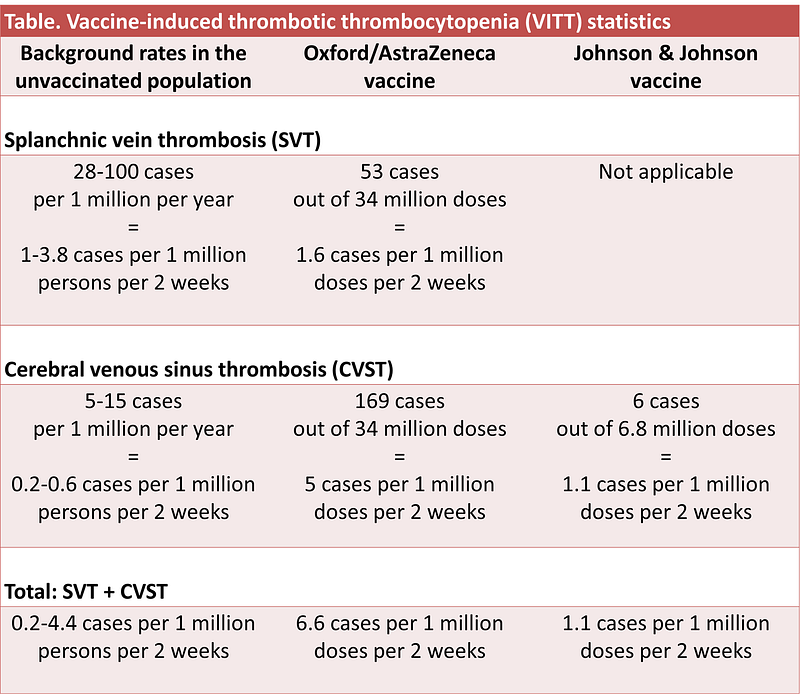
As of 4 April 2021, 34 million persons in the U.K. and Europe have taken the Ox/AZ vaccine, of whom 169 and 53 persons developed cerebral venous sinus thrombosis (CVST) and splanchnic vein thrombosis (SVT), respectively. These cases happened mostly to women younger than 60 years and within two weeks of vaccination. As of 22 March 2021, 14 out of 62 CVST and 4 out of 24 SVT cases ended in death.
CVST is a rare type of stroke, where blood clots develop in the vein in the brain, hindering blood flow. In SVT, this happens in the vein in the abdomen. Both CVST and SVT are thrombotic (blood clot) disorders. But what makes the vaccine-associated CVST and SVT cases unique is that they are also accompanied by thrombocytopenia (low platelets). So, scientists call these cases vaccine-induced thrombotic thrombocytopenia (VITT).
(Platelets — or thrombocytes — are cells that clot blood, usually to prevent bleeding when blood vessels are injured. When excessive blood clots occur, platelet count drops as they are being used up for the blood clot.)
It’s vaccine-induced because these cases of blood clots, particularly CVST, do not happen coincidentally with the vaccine. One way scientists know this is by comparing the incident rates in the vaccinated vs. unvaccinated groups:
As a result, many countries have restricted using the Ox/AZ vaccine to the older age groups at greater risk for severe and fatal Covid-19. Denmark has even discarded the Ox/AZ vaccine entirely. The U.S. is donating unused Ox/AZ vaccines to India who is currently facing a Covid-19 crisis. And the European Medicines Agency (EMA) confirmed VITT as a possible rare side effect of the Ox/AZ vaccine on 7 April 2021.
Soon on 13 April 2021, the U.S. CDC and FDA suspended the use of the J&J DNA vaccine, which is also adenoviral vectored like the Ox/AZ DNA vaccine. Six CVST cases — all in women aged 18–48 years — occurred within 6–13 days of receiving the J&J vaccine out of the 6.8 million doses given, and one died.
As this rate is higher than what is expected from the unvaccinated group (see the table above for CVST), the EMA “concluded that a warning about unusual blood clots with low blood platelets should be added” to the J&J vaccine. But because the benefits of the single-dose J&J vaccine outweigh its risks, the CDC and FDA have lifted their suspension on 23 April 2021.
So, it’s evident that the Ox/AZ and J&J adenoviral-vectored DNA vaccines can trigger blood clots (thrombosis) and low platelets (thrombocytopenia) — hence, the name VITT — in rare instances at <10 cases per million doses.
Possible signs of VITT are shortness of breath, chest pain, leg swelling, persistent abdominal pain, neurological symptoms (e.g., severe headaches and blurred vision), and blood spots under the skin beyond the injection site. The EMA advises that people who see these signs within 2–3 weeks of vaccination seek medical attention. VITT can be prevented if treated early with intravenous gamma globulin — i.e., antibodies that block the blood clot-causing antibodies— followed by non-heparin anticoagulants.

Possible underreporting?
Thus far, surveillance systems have only picked up VITT cases among young people. This could mean that VITT incidents among the older groups might have been overlooked. “Blood clots and strokes are more common in older people, and might not trigger the same in-depth investigation that blood clots in younger vaccine recipients would,” Nature news reported.
An editorial in the New England Journal of Medicine has also stated that “These numbers [of VITT cases] may be underestimates, since reporting is voluntary.” Sebastian Rushworth, MD, agrees that vaccine side effects are often not reported because it has to pass three steps: The clinician has to know that the patient has received the Covid-19 vaccine, suspect that it’s a vaccine side effect, and report to authorities.
A true VITT incident in an older person may be missed in the second step. The third step is also easily missed; drug side effects are always recorded in the patient’s records but not necessarily to external agencies.
A 2006 systematic review of 37 studies estimated that as many as 90% of drug side effects were not reported unless investigations were conducted, but only two studies looked at vaccines. One study found 6% of polio vaccine-related paralytic poliomyelitis cases were not reported. In the other study, 82% of immune thrombocytopenia cases from the measles, mumps, and rubella vaccine were found unreported to authorities.
However, Covid-19 vaccines have garnered global attention, and experts are always looking out for their true side effects. So it’s doubtful that the difference between true and reported cases of VITT would vary a lot.
What’s happening at the biological level
Such VITT cases have not happened with the Pfizer-BioNTech and Moderna vaccines that use the messenger RNA (mRNA) technology. (But cases of low platelets without blood clots have occurred with the mRNA vaccines at the rate of 1 case per million doses.) This suggests that VITT may have something to do with what Ox/AZ and J&J vaccines have in common.
The Ox/AZ and J&J vaccines both use a harmless adenovirus as a vector or carrier to deliver the DNA (that encodes the spike protein of SARS-CoV-2) into human cells. The cell first converts the DNA into mRNA and translates the mRNA into the spike protein. The immune system then reacts against and forms a memory of the spike protein. This memory readies the immune system to act swiftly should it reencounters the spike protein in the future, such as during a SARS-CoV-2 infection.
The only difference is that the Ox/AZ uses a chimpanzee adenovirus, whereas the J&J uses human adenovirus type 26 (Ad26). Both adenoviruses are genetically modified to remove their genomes, so they can’t replicate inside cells as normal viruses would.
In four timely studies published this month in the New England Journal of Medicine, researchers from Germany, Norway, the U.K., and the U.S. shed light on what might be happening at the biological level during VITT.
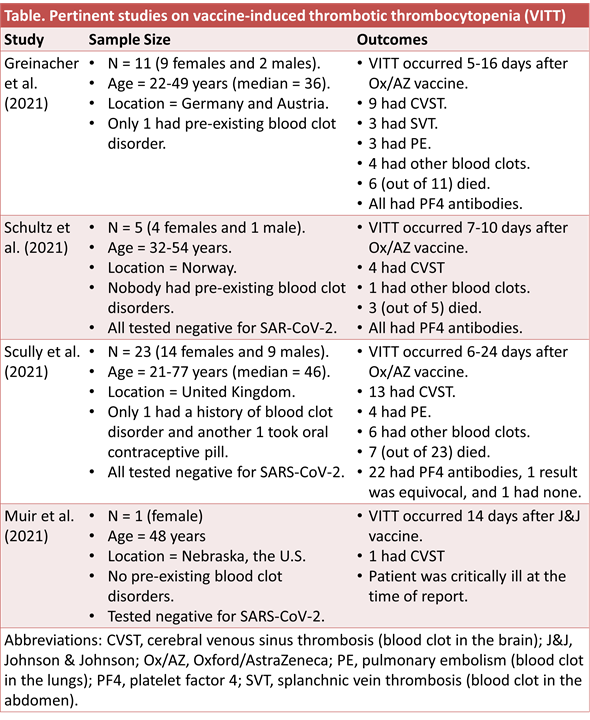
The studies found evidence of antibodies targeting the platelet factor 4 (PF4) in nearly all the patients. Although most of the patients in these studies took Ox/AZ vaccine, with only one case study with the J&J vaccine, the U.S. Advisory Committee on Immunization Practices has reported that 5 out of 6 Americans who developed VITT from the J&J vaccine had PF4 antibodies.
Antibodies targeting PF4 — i.e., PF4 antibodies — activate platelets. And when there are too many PF4 antibodies floating around in the bloodstream, excessive blood clots and a massive drop in free platelets will occur. (Because platelets are being used up for the blood clot.)
As seen in the table, VITT normally occurs about a week after vaccination. This is because the adaptive immune system — including B-cells that make antibodies — takes about a week to activate.
The fact that PF4 antibodies were detected in nearly all the VITT cases suggests a causal link — that the vaccine is causing these problems. But because VITT is so rare, there isn’t enough statistical power to prove causality, argued two commentaries in the British Medical Journal. At the same time, however, we see a spike in such a rare medical phenomenon not seen before, which there’s no other plausible reason besides the Ox/AZ vaccine.
Why does the immune system make PF4 antibodies in response to the Ox/AZ and J&J vaccines? The researchers think it’s because the adenovirus vector interacted with platelets. They cited studies showing that adenovirus used for gene delivery — not the same type as the Ox/AZ and J&J vaccines — could bind to and activate platelets, triggering blood clots and low platelets in animals. Scientists that did such animal studies have even said that they were not surprised about the link between VITT and adenovirus-based vaccines.
This theory is in line with the one proposed by Hamid A. Merchant, Ph.D., a pharmaceutical researcher at the University of Huddersfield in England, in his letter to the British Medical Journal. He theorized that the vaccine might have ‘infected’ the platelets. The immune system might then see the ‘infected’ platelets as foreign and attack them.
How did the vaccines end up interacting with the platelets? Scientists have argued that the gene delivery technology used by genetic vaccines — such as the Ox/AZ and J&J vaccines — has a broad tissue distribution. This means that the genetic vaccine may be carried into other tissues or cells beyond the injection site, which may include platelets. But this usually happens with a tiny amount of vaccine particles, as shown in animal studies. So its clinical consequences may be negligible, as detailed thoroughly here:
But outliers are bound to happen by chance, which may lead to VITT. Thus, VITT can be considered as a form of vaccine’s off-target effects on the platelets that occur by chance. With the current VITT statistics, this chance is a few times (less than 10, to be generous) in a million.
VITT happens more often in females than males may be due to differences in immunological strength. Biologically, females have XX chromosomes while males have XY. As most immune system-related genes are located on the X-chromosome, females generally mount stronger immune reactions. Although this helps them fight infections better, it comes at the costs of increased risk of autoimmune problems, which may include VITT. But there could also be other genetic, hormonal, or environmental factors to VITT that are yet to be pinpointed.
The risk-benefit judgment
The EMA and other authorities have concluded that the benefits of the Ox/AZ and J&J vaccines in protecting against Covid-19 outweigh the risks of VITT. Covid-19 causes blood clots in the lungs (pulmonary embolism) and legs (venous thromboembolism; VTE) — in 8% and 11% of patients, respectively. Although VTE is not VITT or CVST, it can be fatal as well.
Another common statistics comparison is with the oral contraceptive pill that causes 300–900 cases of VTE per million users annually. Air travel can also cause VTE at the rate of 3000 cases per million per year.
But whether one should take the Ox/AZ or J&J vaccine really depends on the risk-benefit analysis for a specific situation.
In Australia, for example, where Covid-19 cases remain low, young people may be better off waiting for another vaccine. In countries where Covid-19 cases remain high, the risk-benefit analysis is more dilemmatic. In the U.K., the risk of serious harm from the vaccine among the 20–29 years-olds is about 1.1 in 100,000, according to the calculations of David Spiegelhalter, a statistician professor at the University of Cambridge. The risk of intensive care unit admission due to Covid-19 among the 20–29 years-olds, on the other hand, ranges from 0.8 to 6.9 in 100,000 persons.
“In this sort of gradual sliding curve of benefit-risk balance, there’s no sudden point at which it becomes safe or unsafe,” Prof. Spiegelhalter said. But the professor thinks that the vaccine is a net benefit for the population because getting vaccinated protects others from Covid-19 via herd immunity. “I think that’s an aspect that has not been emphasized enough,” the professor said.
For the not-so-well-off countries that don’t have enough vaccines to protect themselves against the spreading Covid-19, the situation is again different. This is especially tragic for India that is now facing a Covid-19 crisis, with over 2000 deaths per day. In such countries, any kind of vaccine with an acceptable safety profile and decent efficacy will help, even in the younger populations. There’s no room for being picky if there are no alternative vaccines to choose from.
Closing remarks
VITT took us by surprise. It’s no wonder that it did because VITT was an alien medical term until this month. Not to mention that VITT is very unusual in that it has to fulfill four conditions:
- The use of adenovirus-vectored DNA technology, such as the Ox/AZ and J&J vaccines for Covid-19. (This also means that VITT can happen with vaccines using similar technology, such as Sputnik V and Convidecia.)
- The random or chance occurrence of vaccine’s off-target effects on the platelets, unless certain genetic factors are identified in the future.
- The misfiring of the immune system that deploys a huge number of PF4 antibodies against the platelets.
- A surveillance and reporting system that is robust enough to pick up very rare medical conditions that might have been missed if it wasn't for the pandemic that has gathered our global attention.
VITT incidents that pass these conditions ultimately amounted to <10 cases for every million doses of Ox/AZ or J&J vaccine shot. What this number means for you depends on the Covid-19 situation your region is facing.
If you have made it this far, I appreciate it. Subscribe to my Medium email list here. If you want to become a member to get unlimited access to Medium, you can use my referral link and I will receive a small commission.





