
The Cognitive Model of Psychopathology: Characteristic Errors in Information Processing
We can see that there are many ways in which we actively contribute to our own experience of mental unrest and suffering. — Dalai Lama

The cognitive model for psychopathology is grounded on the theory that there are characteristic errors in information processing in depression, anxiety disorders, personality disturbances and other psychiatric conditions (Beck, 1976; Beck & Rush, 1994). Additionally, individuals possess a set of idiosyncratic vulnerabilities and sensitivities which are manifestations of their cognitive structures and which predispose them to specific psychological distress elicited by the perception of threat. Viewed from the cognitive perspective an individual’s personality is shaped by the central values known as super-ordinate schemas and psychological distress is caused by a characteristic maladaptive response to specific stressors based on the individual’s learning history (Corsisni & Wedding, 1989).
Psychopathology, then, exists along the same continuum as normal emotional reactions but is manifested in exaggerated, overly intense, rigid and/or inappropriate responses. Normal reactions are mediated by cognitive processes that enable individuals to perceive reality accurately and respond with appropriate behavior. In instances of psychopathology this mechanism is impaired and corresponding cognitive errors occur thus skewing the interpretation of experience and producing negative schemas that persist even despite contradictory evidence Kaplan & Saddock, 1991).
Ideally an individual perceives situations accurately, interprets them correctly, and consequently manifests cognitive, emotional, and behavioral responses which are appropriate to the situation and which prove to be adaptive. According to the cognitive model, on those occasions when the individual’s perception of the situation is biased or in which the perceived situation is interpreted incorrectly, the cognitive, emotional and/or behavioral responses will be inappropriate to the situation or maladaptive to some extent. However, in most situations the individual’s perception and interpretation of subsequent events will provide feedback which reveals the extent to which the responses were inaccurate or maladaptive. Once this feedback is accurately perceived and interpreted, it not only corrects the specific misperceptions and misinterpretations which occurred but is also stored in memory to aid in accurately perceiving and interpreting future events (Pretzer & Beck, 1996).
Thus, the cognitive view maintains that, given the complexity of daily life and the ambiguity of many interpersonal interactions, occasional misperceptions and misinterpretations of events are inevitable. However, isolated misperceptions and misinterpretations give rise to isolated maladaptive responses which are easily corrected by subsequent experiences. In order for seriously maladaptive responses to develop, a systematic bias in perception, recall, or interpretation — more serious and persistent than that which would result from normal misperceptions and misinterpretations — is required. Furthermore, a distortion in the feedback process either by strongly biasing the interpretation of events or by influencing the responses of others, will result in persistent maladaptive responses. According to the cognitive perspective, each psychopathological disorder maintains its own specific cognitive profile of distorted thoughts, which, when analyzed provides the framework for therapeutic interventions. (See Table 1).
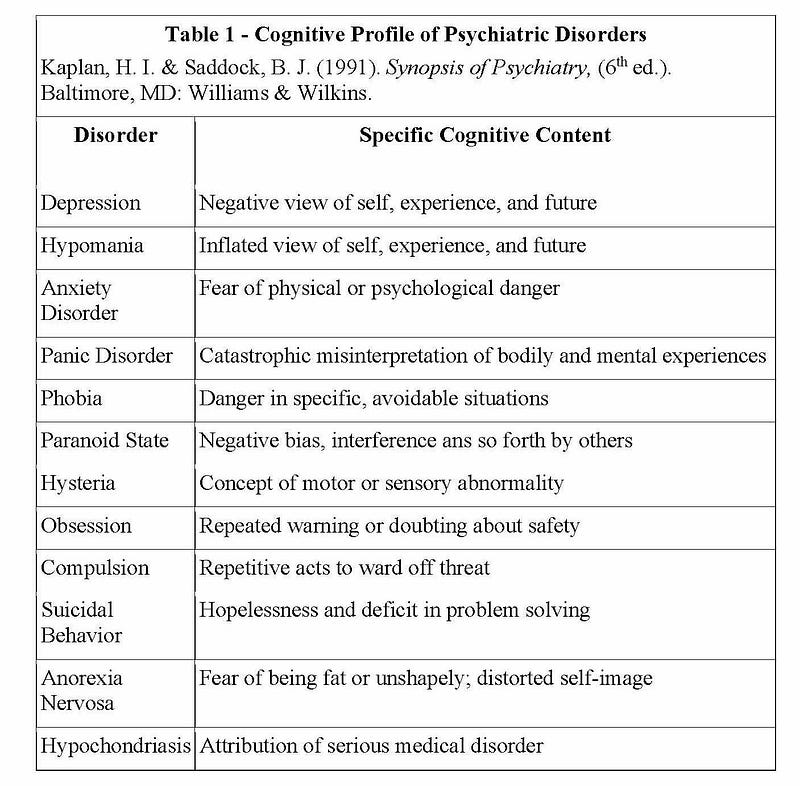
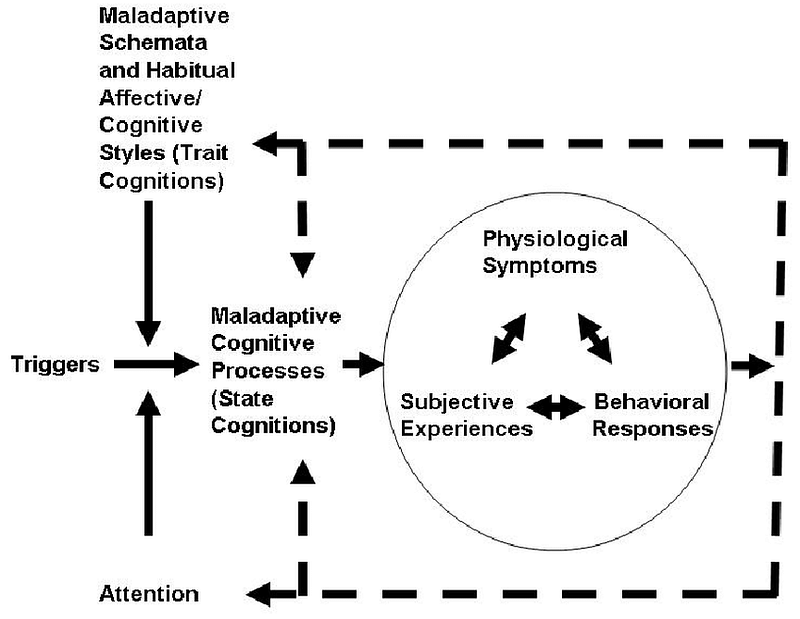
Because the individual’s schemas, beliefs, and assumptions have a major impact on the perception, recall and interpretation of events, they represent one possible source of such systematic bias. However, the cognitive model focuses on the interplay between the many nuances of cognition, affect, and behavior in the development and/or maintenance of psychopathology (see Figure 1). The individual’s beliefs and assumptions have impact on the perception of events and on interpersonal behavior and, reciprocally, an individual’s interpersonal behavior influences the responses of others which, in turn, result in experiences that influence the first individual’s beliefs and assumptions. Particular interpersonal behavior may provoke subsequent reactive behavior and/or elicit certain treatment from others that provides additional experiences which seem to confirm the initial negative or inappropriate perception (Pretzer & Beck, 1996).
Figure 1 — The Role of Cognition in Psychopathology
Furthermore, while the cognitive model assumes that the individual’s interpretation of events shapes the emotional response to the situation, it also argues that the individual’s emotional state has important effects on cognition. Research has demonstrated that affect tends to influence both cognition and behavior in mood-congruent ways (Isen,1984). A number of studies have corroborated that even a mild, experimentally induced depressed mood biases perception and recall in a depression-congruent way (Watkins, Mathews, Williamson, & Fuller, 1992). Thus, for example, a depressed mood increases the likelihood that the individual will focus on negative aspects of the situation and preferentially recall negative experiences which occurred in the past.
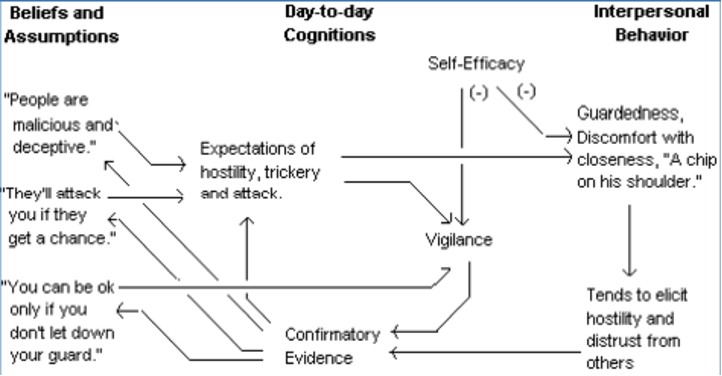
Similarly, as an individual’s level of anxiety increases, attentional processes appear to be biased in favor of signs of threat (Watkins, et al., 1992). This phenomenon lays the foundation for a potentially self-perpetuating cycle where the individual’s automatic thoughts elicit a particular mood, the mood biases perception and recall in a mood-congruent way, thus increasing the likelihood of additional mood-eliciting automatic thoughts, which elicits more of the mood in question, further biasing perception and recall, and so on until something happens to disrupt the cycle (Pretzer & Beck, 1996). See Figure 2.
Figure 2 — Cognitive Conceptualization of Paranoid Personality Disorder
Affect can play an important role in an individual’s functioning in another way as well. As Taylor and Rachman (1991,1992) have noted, individuals may fear certain emotions and may strive to avoid the emotion itself, may seek to escape from experiencing the emotion as quickly as possible, or may attempt to avoid thoughts, memories, or situations which they expect to elicit the emotion. This type of self-perpetuating cognitive-interpersonal cycle can be quite persistent and resistant to change. Once such a pattern is established, the individual’s schemas tend to bias the perception of events in such a way that experiences which otherwise would contradict the faulty assumptions are overlooked, discounted, or misinterpreted while, at the same time, this interpretation of events and the corresponding interpersonal behavior result in experiences which seem to confirm the dysfunctional schemas (Pretzer & Beck, 1996).
References
Beck, A. T. (1976). Cognitive therapy and the emotional disorders. New York, NY: International Universities Press.
Beck, A. T., Rush, A. J. (1994). In Kaplan, H. I. & Saddock, B. J. (Eds). Comprehensive
textbook of psychiatry, (6th ed.). Baltimore, MD: William & Wilkins.
Corsini, R. J. & Wedding, D. (2018). Current psychotherapies, (4th ed.). Boston, MA: Cengage.
Isen, A.M. (1984). Toward understanding the role of affect in cognition. In R.S. Wyer & T.K. Skrull (Eds.). Handbook of social cognition. Hillsdale, N.J.: Lawrence Erlbaum.
Kaplan, H. I. & Saddock, B. J. (1991). Synopsis of Psychiatry, (6th ed). Baltimore, MD: Williams & Wilkins.
Pretzer, J.L. & Beck, A.T. (1996). A cognitive theory of personality disorders. In: J.F. Clarkin & M.F. Lenzenweger (Eds.) Major Theories of Personality Disorder. New York, NY: Guilford.
Taylor, S., & Rachman, S.J. (1991). Fear of sadness. Journal of Anxiety Disorders, 5: 375–381.
Taylor, S., & Rachman, S.J. (1992) Fear and avoidance of aversive affective states: Dimension and causal relations. Journal of Anxiety Disorders, 6: 15–25.
Watkins, P.C., Mathews, A., Williamson, D.A., & Fuller, R.D. (1992). Mood-congruent memory in depression: Emotional priming or elaboration? Journal of Abnormal Psychology, 101: 581–586.





