
mRNA Vaccine Safety and Risks: A One-Year Update From the U.S., U.K., and Israel
Although new risks of mRNA vaccines have been discovered, they are not a cause for alarm.

It has been almost a year since the BioNTech-Pfizer’s and Moderna’s mRNA vaccines received emergency use authorization (EUA) from the Food and Drug Administration (FDA) for public use amidst the Covid-19 pandemic in December 2020. These two vaccines are the earliest ones we started using, so they have also been studied very closely.
At present, the FDA has given the first full approval for Pfizer’s mRNA vaccine. Three massive studies on mRNA vaccine safety were also published during the past month, which have made important and somewhat unpleasant discoveries. Let’s see what they are with a critical eye.
1. Data from Israel (Pfizer’s mRNA vaccine)
In a population-based observational study published in the New England Journal of Medicine on 25 August 2021, titled “Safety of the BNT162b2 mRNA Covid-19 Vaccine in a Nationwide Setting,” researchers from Israel capitalized on the Clalit Health Services database that contains medical data of 52% of Israel’s population (>4.7 million out of 9 million persons).
They carefully matched 884,828 vaccinated (with Pfizer’s mRNA) with 884,828 unvaccinated (control) individuals. Both groups are nearly identical in age, sex, residence, socioeconomic status, population sector, and number and type of preexisting chronic conditions.
This matching ensures whatever differences observed between the two groups were most likely due to the mRNA vaccine. The differences they investigated are 25 adverse events —as reported to surveillance systems like the Vaccine Adverse Event Reporting System (VAERS) — that may occur within 21 days of either the first or second vaccine dose. (For more info on what VAERS serves to do, see here.)
The 25 adverse events are:
1. Acute kidney injury 2. Anemia: low red blood cells 3. Appendicitis: swollen and inflamed appendix 4. Arrhythmia: heart rhythm problems 5. Arthritis or arthropathy: joint problems 6. Bell’s palsy: facial muscle weakness or paralysis 7. Cerebrovascular accident: stroke 8. Deep-vein thrombosis: blood clot in the leg vein 9. Herpes simplex infection: blisters, usually at the mouth 10. Herpes zoster infection: skin rashes or shingles 11. Intracranial hemorrhage: bleeding in the brain 12. Lymphadenopathy: enlarged lymph nodes 13. Lymphopenia: low white blood cell count 14. Myocardial infarction: heart attack 15. Myocarditis: inflamed heart muscle 16. Neutropenia: low neutrophil, a type of white blood cell, count 17. Other thromboses: other blood clots in intestines, liver, or brain 18. Paresthesia: prickling sensation in hands or feet 19. Pericarditis: inflamed heart outer linings 20. Pulmonary embolism: blood clots that travel from legs to lungs 21. Seizure: overactive neurons that can disrupt muscle tone 22. Syncope: faint or pass out 23. Thrombocytopenia: low platelets that can cause excessive bleeding 24. Uveitis: inflamed eyes 25. Vertigo: balance problems
This study did not consider common vaccine side effects— such as fever, malaise, and injection site pain — as potential vaccine-related adverse events.
The study computed their analyses in risk ratio (RR) and risk difference (RD). RR is relative (e.g., 5%÷10% = ↓ 50% or 0.1%÷0.2% = ↓ 50%), whereas RD is absolute (e.g., 5%−10% = −5% or 0.1%−0.2% = −0.1%).
As you can see, RR can be misleading sometimes; after all, a rare event compared to a rare event will still be a rare event. So, when looking at rare events, RD is the better number to look at.
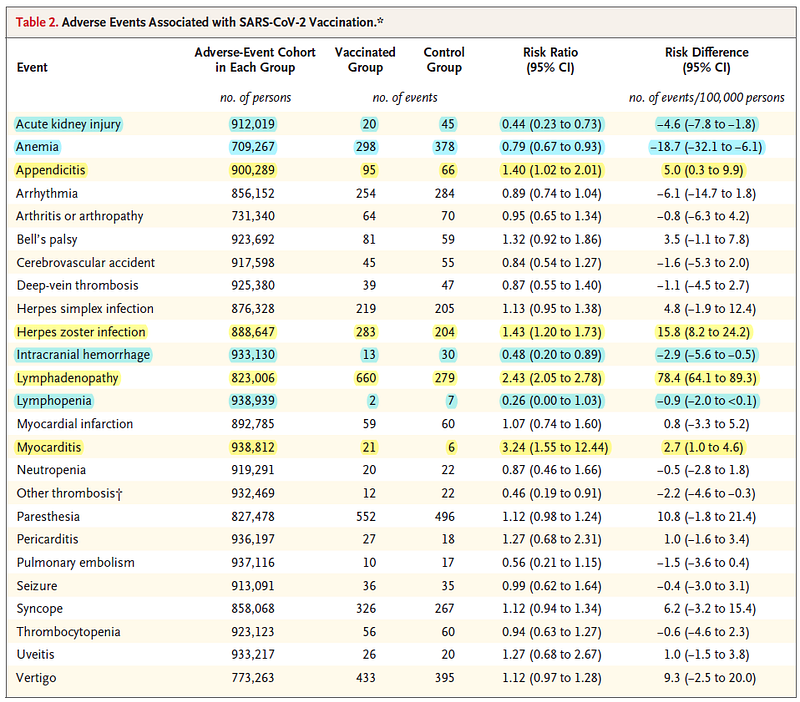
Results revealed that compared to the unvaccinated group, the vaccinated group had higher risks of:
- Myocarditis (inflamed heart muscle): RR = 3.24-times increased risk; RD = 2.7 excess events per 100,000 persons. For this adverse event, 90% of the cases are males aged 20–34 years.
- Lymphadenopathy (enlarged lymph nodes): RR = 2.43-times increased risk; RD = 78.4 excess events for 100,000 persons.
- Appendicitis (swollen appendicitis): RR = 1.4-times increased risk; RD = 5 excess events per 100,000 persons.
- Herpes zoster infection (skin rashes or shingles): RR = 1.43-times increased risk; RD = 15.8 excess events per 100,000 persons.
Interestingly, the vaccinated group had lower risks of anemia (1.2-times decreased risk; 18.7 fewer events per 100,000 persons), acute kidney injury (1.6-times decreased risk; 4.6 fewer events), intracranial hemorrhage (1.5-times decreased risk; 2.9 fewer events), and lymphopenia (1.7-times decreased risk; 0.9 fewer events) compared to the unvaccinated group.
Why the mRNA vaccine protects against these adverse events is unknown, but it’s probably due to the general immune reactions rather than the vaccine itself. And the same could be said for the four adverse events (in bulleted points above) that the vaccine likely causes.
For the remaining 17 adverse events, there were no significant differences in incidence rates between vaccinated and unvaccinated groups. This means that despite being reported to surveillance systems, these 17 adverse events are just coincidences that would have happened without the vaccines.
And the authors compiled their results nicely in this table:
Moving on, this study also did the same matched comparison for 173,106 SARS-CoV-2-infected and 173,106 uninfected persons. And they found increased risks of the following in the SARS-CoV-2-infected group:
- Myocarditis (inflamed heart muscle): RR = 18.3-times increased risk; RD = 11 excess events per 100,000 persons.
- Acute kidney injury: RR = 14.8-times increased risk; RD = 125.4 excess events per 100,000 persons.
- Pulmonary embolism (blood clots in the lungs): RR = 12.1-times increased risk; RD = 61.7 excess events per 100,000 persons.
- Intracranial hemorrhage (bleeding in the brain): RR = 6.9-times increased risk; RD = 7.6 excess events per 100,000 persons.
- Pericarditis (inflamed heart outer linings): RR = 5.4-times increased risk; RD = 10.9 excess events per 100,000 persons.
- Myocardial infarction (heart attack): RR = 4.5-times increased risk; RD = 25.1 excess events per 100,000 persons.
- Deep-vein thrombosis (blood clots usually in the leg): RR = 3.8-times increased risk; RD = 43 excess events per 100,000 persons.
- Arrhythmia (irregular heart rhythm): RR = 3.8-times increased risk; RD = 166.1 excess events per 100,000 persons.
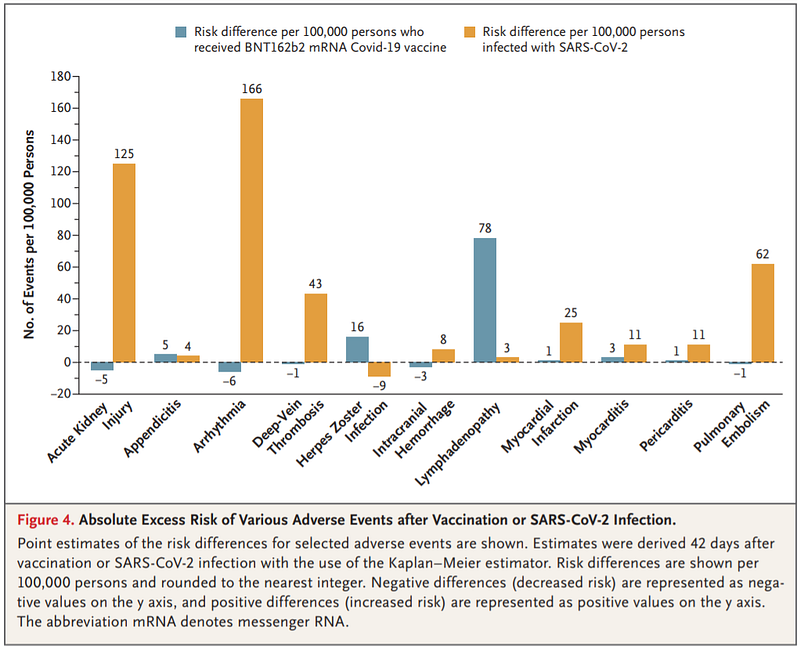
The study authors then compared the RD of the adverse events faced by the vaccinated (vs. unvaccinated) and infected (vs. uninfected) groups. As shown in the figure below, infected people experienced much more adverse events (about 10–100-times more) than vaccinated people — except for herpes zoster infection and lymphadenopathy only.
The observation that SARS-CoV-2 infection can increase the risks of other diseases or disorders is not surprising, as other studies have also found.
2. Data from the U.S. (Pfizer’s and Moderna’s mRNA)
In a paper published in the Journal of American Medical Association (JAMA) on 3 September 2021, titled “Surveillance for Adverse Events After COVID-19 mRNA Vaccination,” researchers from the U.S. did a similar population-based, observational study.
Using the Vaccine Safety Datalink (VSD) that stores health data of about 12.5 million Americans (3.6% of the U.S. population), this study matched vaccinated (within 21 days of receiving a dose of Pfizer’s or Moderna’s vaccine) to two comparators in terms of age, sex, race, ethnicity, and region. The two comparators are unvaccinated and vaccinated (at 22–42th day of vaccination) people.
This study compared vaccinated people at 0–21th vs. 22–42th day after vaccination because “individuals with recent vaccination were expected to be more similar to those with more remote vaccination than they were to unvaccinated individuals,” the study authors explained.
After consultation among the Centers for Disease Control and Prevention (CDC), Food and Drug Administration (FDA), Department of Defense, and Department of Veteran Affairs, this study looked for 23 adverse events that might be linked to the mRNA vaccines:
1. Acute disseminated encephalomyelitis: inflamed brain and spinal cord. 2. Anaphylaxis: severe allergic reaction. 3. Encephalitis/myelitis: inflamed membrane of the brain/spinal cord. 4. Guillain-Barré syndrome: autoimmune disorder attacking nerves. 5. Immune thrombocytopenia: autoimmune disorder attacking platelets. 6. Kawasaki disease: unusual high fever that’s persistent. 7. Narcolepsy: brain disorder that causes involuntary, sudden sleep. 8. Seizures: overactive neurons that can disrupt muscle tone. 9. Transverse myelitis: inflamed spinal cord. 10. Appendicitis: swollen and inflamed appendix. 11. Bell’s palsy: facial muscle weakness or paralysis. 12. Acute myocardial infarction: heart attack. 13. Acute respiratory distress syndrome: severe lung injury. 14. Disseminated intravascular coagulation: widespread blood clots. 15. Multisystem inflammatory syndrome in children and adults. 16. Myocarditis/pericarditis: inflamed heart tissues. 17. Pulmonary embolism: blood clots that travel from legs to lungs. 18. Hemorrhagic and ischemic stroke: disrupted blood supply to the brain. 19. Thrombotic thrombocytopenic purpura: widespread small blood clots. 20. Venous thromboembolism: blood clots in veins, typically in the legs. 21. Cerebral venous sinus thrombosis: blood clots in the brain. 22. Thrombosis with thrombocytopenia syndrome: blood clots with low platelets that can cause excessive bleeding. 23. Younger subgroup of myocarditis/pericarditis: inflamed heart tissues.
Among the 23 adverse events investigated, only two reached statistical significance. One is anaphylaxis with an excess of about 5 cases per 1 million doses. Most of those anaphylaxis cases occurred within 30 minutes of vaccination; 95% of cases affected females; 78% had an allergy history.
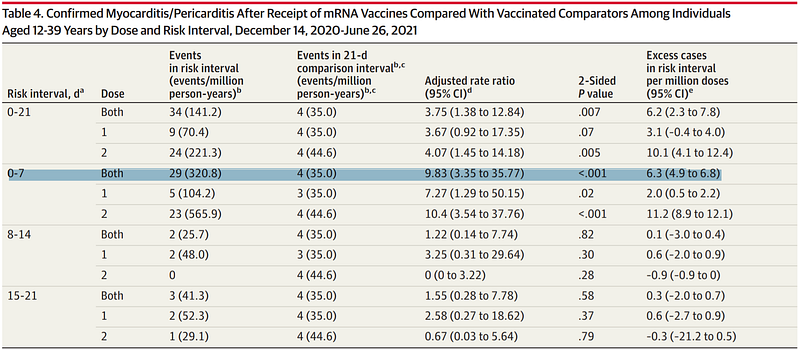
The second is the younger subgroup of myocarditis/pericarditis. Specifically, 12–39-year-olds at days 1–21 of vaccination had a 9.8-times increased risk of myocarditis or pericarditis compared to those at days 22–42 of vaccination. This gives an excess of 6.3 cases per million doses.
More specifically, 85% were male, 85% experienced it within 7 days of vaccination, 82% were hospitalized, and 6% were admitted to the intensive care unit. But nobody died.
Why vaccine-related myocarditis/pericarditis only affected the younger age group is unclear. Experts believe it’s due to excessive inflammation from the vaccine immune response. One interesting hypothesis I learned from an email conversation is that younger people, especially males, have faster metabolism that might overly metabolize the mRNA vaccine, creating more spike proteins that might become inflammatory. After all, the mRNA (and DNA) vaccine is a novel technology that relies on the body to produce the spike proteins. Older vaccine technology, in contrast, injects a set amount of immunogen — that is, the spike proteins or inactivated virions in this case.
3. Data from the U.K. (AstraZeneca’s DNA and Pfizer’s mRNA vaccines)
In a study published in the British Medical Journal (BMJ) on 27 August 2021, titled “Risk of thrombocytopenia and thromboembolism after covid-19 vaccination and SARS-CoV-2 positive testing: self-controlled case series study,” researchers from the U.K. performed another population-based, observational study but with slightly dissimilar design to the ones from Israel and the U.S.
As stated in the title, this study’s design is self-controlled case series. This means the vaccinated/unvaccinated and infected/uninfected groups consist of the same individuals at different time points — such as pre- and post-vaccination (from AstraZeneca’s DNA or Pfizer’s mRNA) and pre- and post-infection (from SARS-CoV-2). This design has its perks in that it controls for nearly all variables that could have differed from person to person.
Based on the blood clots concerns surrounding the Covid-19 vaccines for some time already, this study investigated whether any of the following disorders are actually linked to the vaccine:
1. Thrombocytopenia: low platelets that can cause excessive bleeding. 2. Venous thromboembolism: blood clots in veins, typically in the legs. 3. Arterial thromboembolism: blood clots in arteries, typically in the legs. 4. Cerebral venous sinus thrombosis: blood clots in the brain. 5. Ischaemic stroke: blood clot impeding blood flow to the brain. 6. Myocardial infarction: heart attack. 7. Other rare blood clotting diseases.
This study used the National Immunisation Management System that stores data of 29.1 million persons in England who received their first doses of either AstraZeneca’s DNA (19.6 million) or Pfizer’s mRNA (9.5 million) vaccines to determine the incidence rates of those seven diseases following vaccination. Of the 29.1 million individuals, 1.8 million also received a positive SARS-CoV-2 test, and the incidence rates of those diseases were also computed.
Such rates are then compared with their pre-vaccination, pre-infection, or pre-pandemic (2015–2019) rates. The pre-pandemic rates were calculated from the QResearch database of 12 million patients.
Results revealed that compared to the pre-vaccination or pre-infection period, those who later got the Pfizer’s mRNA vaccine, AstraZeneca’s vaccine, or SARS-CoV-2 infection were at increased risks of:
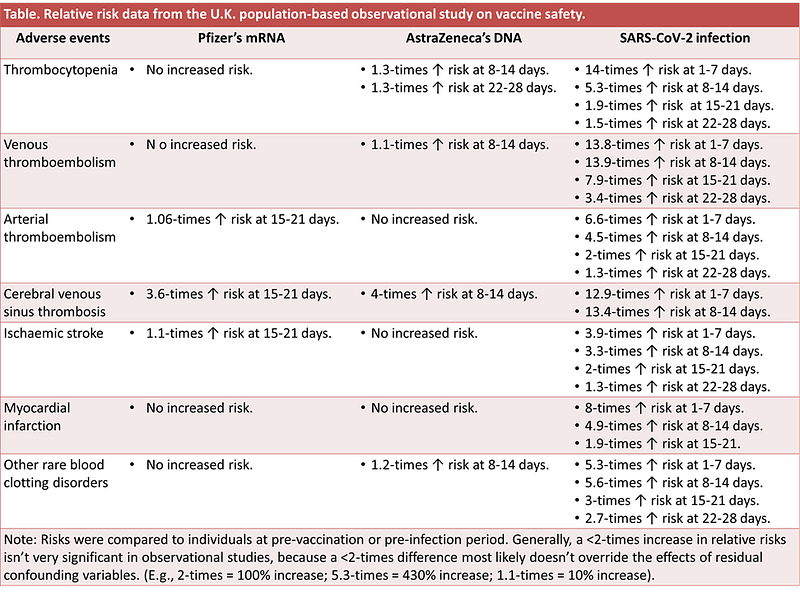
So, AstraZeneca’s DNA vaccine is associated with a small increased risk of thrombocytopenia, venous thromboembolism, cerebral venous sinus thrombosis (CVST), and other rare blood clotting disorders. And Pfizer’s mRNA vaccine with arterial thromboembolism, CVST, and ischaemic stroke.
These relative risks are considered small because they are less than 2-times. Generally, in observational studies, a less than 2-times difference are unlikely to override the effects of residual, uncontrolled confounding factors — such as genetics, socioeconomic status, or health awareness.
This is except for CVST with ~4-times increased risk. But as mentioned in the first section above, a rare event compared to a rare event will still be rare. Thus, the relative risk (RR) of CVST doesn't inform much about the real-world context. Yes, CVST is very rare. In this study, they were only 75 CVST cases out of 29.1 million vaccinated persons.
Thankfully, this study did compute the risk difference (RD) for some of the adverse events that reached statistical significance for RD:
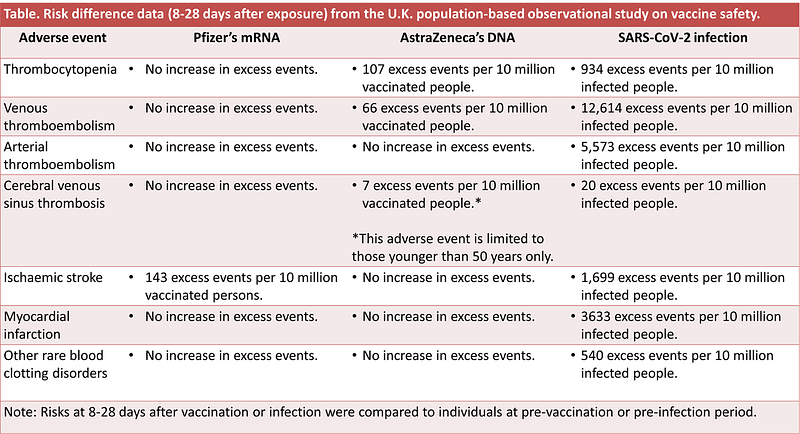
Evidently, for the SARS-CoV-2-infected group, the RR and RD numbers were many times higher than the vaccinated group. This makes the risks of those adverse events in the vaccinated group pale in comparison.
What makes these studies valuable
Based on the three population-based, observational studies from Israel, the U.S., and the U.K., we cannot deny that mRNA and DNA vaccines have their risks (although much lower than that of SARS-CoV-2 infection) that were not detected from their previous clinical trials.
Overall, the Pfizer’s mRNA vaccine has most likely caused a small-to-moderate increase in excess cases of myocarditis (inflamed heart muscle), pericarditis (inflamed heart’s outer linings), lymphadenopathy (enlarged lymph nodes), appendicitis (swollen appendicitis), herpes zoster infection (that causes skin rashes), anaphylaxis (severe allergic reaction), and ischaemic stroke (blood clots blocking the blood supply to the brain).
It’s most likely because observational studies can’t prove causation; only randomized controlled trials (RCTs) can. Randomization means individuals are assigned to either the experimental/study or comparison/control group randomly. Such randomization controls or negates the countless variables that differ between people, which may influence the study’s outcome of interest. So, observational studies without randomized groups cannot possibly control every factor that may have affected the results — such as genetics and environmental factors. Observational studies usually control for controllable factors only — such as age, sex, and underlying medical conditions.
(Since we know that the mRNA and DNA vaccines work from the previous RCTs, it’s unethical to inject people with placebo now to determine if the vaccine really caused those adverse events).
Some of these excess events — especially myocarditis, pericarditis, and blood clot disorders — have hospitalized people. A tiny proportion of those hospitalizations might have even ended up in death — especially from blood clot disorders — as the U.K. study has found. But the cause-and-effect here is uncertain due to the lack of statistical power. It’s difficult to know for sure if a few cases of deaths from vaccine-related adverse events were really due to the vaccine or something else, like genetic factors or other triggers.
Only the U.S. study investigated Moderna’s mRNA vaccine, finding a similar risk profile to Pfizer’s. For AstraZeneca’s DNA vaccine, only the U.K. study examined it and found a higher risk profile than Pfizer’s mRNA vaccine. But the risk profile of SARS-CoV-2 infection is many times higher than the vaccines.
Those three studies, however, only examined short-to-medium-term risks of vaccines. The Israel’s study examined 42 days of follow-up only — 21 days after each of the first and second vaccine doses. The study authors admitted this limitation right away, writing that “adverse events that could not plausibly be diagnosed within 42 days (e.g., chronic autoimmune disease) were not included.” Similarly, the U.S. and U.K. studies only looked at adverse events occurring within roughly a month of vaccination.
That said, those three studies are still precious because they have proper control or comparison groups. Most previous observational studies on vaccine safety monitoring after RCTs don’t have control groups, making it difficult to know how much of the differences or outcomes observed were from baseline or background influences.
After nearly a year since mass vaccination began, we now have a better understanding of the mRNA (and DNA) vaccine’s safety profile. Yes, those vaccines have risks. But like any medical intervention, such risks must be weighed against the risks of infection or benefits of vaccination. This risk-benefit assessment may differ substantially in some people, but for the overwhelming majority, vaccines are the more reasonable choice.
For an update on mRNA vaccine-related heart inflammation, see here: Heart Inflammation From mRNA Vaccine: Probable Causes and Precautions.
If you have made it this far, thank you. Subscribe to my Medium email list here. If you want to become a member to get unlimited access to Medium, you can use my referral link, and I will receive a small commission at no extra cost to you. You can also tip me below if you are feeling generous today, and I’ll appreciate it. Paying bills with science writing isn’t easy, so I’ll appreciate any help I can get.




