

Dissecting the RECOVERY Trial Pre-print: Is There Any Fault?
At least I didn’t find anything that’d undermine its breakthrough findings.
The RECOVERY trial of Oxford University reports the first lifesaving drug for severe Covid-19 called dexamethasone, a synthetic corticosteroid. It is arguable the top good news for Covid-19 treatment presently, earning its status as a breakthrough finding. Many health authorities have now endorsed dexamethasone for treating severe Covid-19. For more information on these and how dexamethasone works, please see here:
Researchers of the RECOVERY trial released their pre-print on June 22, titled “Effect of Dexamethasone in Hospitalised Patients with COVID-19: Preliminary Report,” in medrxiv.org. Looking closely at how they conducted the study and their analyses, do the results still stand its breakthrough status? The answer is yes. Let’s move on to the justifications.

METHODS
1. Randomisation
The RECOVERY trial, the authors wrote, is a “randomised, controlled, open-label, adaptive platform trial.”
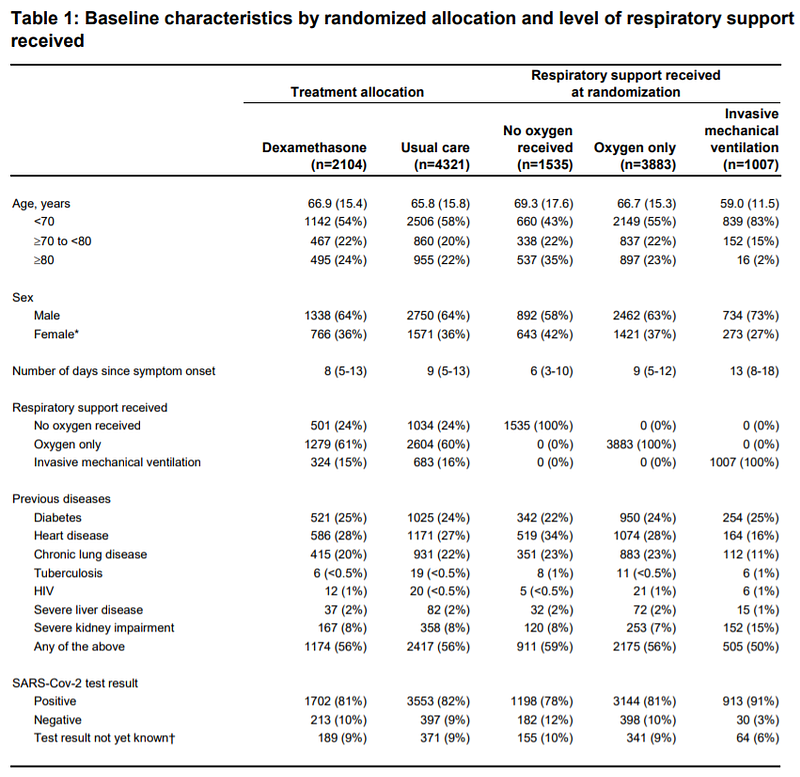
The randomisation and placebo-controlled aspects are robust aspects of the trial. Covid-19 patients either received dexamethasone (6 mg/day orally or intravenously for up to 10 days) or just the standard usual care. Looking at the participants’ baseline characteristics, they are well-balanced in terms of age, sex, comorbidities, etc. (see Table 1). Hence, results derived would not be a consequence of inherent differences between treatment groups.
2. Adaptive Platform
An adaptive platform means that patients’ responses to the treatment are tracked, such as any side effects. Depending on their physiological reactions, the treatment protocol might be modified; often, it is the dosage. Thus, an adaptive clinical trial is a more flexible one, and better reflects real-life clinical practice. Furthermore, the RECOVERY trial has a vast sample size by the thousands, which is deemed more than enough by the Steering Committee.
3. Open-Label
Open-label means that there is no blinding; researchers and participants know which treatment group they are allocated to. As they wrote, “Participants and local study staff were not blinded to the allocated treatment.” While they did not explain why they used open-label, the double-blind design is generally better. It reduces bias in data collection, and placebo effects as both researchers and participants do not know who is in which treatment group.
What are the cons of an open-label design? For one, researchers might not know if placebo effects could occur as patients know if they are receiving the real treatment or not. Biases in data collection might happen, but unlikely in this trial as outcomes are quantitative (i.e., 28-day mortality or duration of the hospital stay), and not qualitative (e.g., patients’ subjective feelings/well-being, etc.). So, is this open-label design a big deal? Not enough to undermine the power of randomisation and other strengths of the trial.
RESULTS
1. 28-day Mortality by Respiratory Support
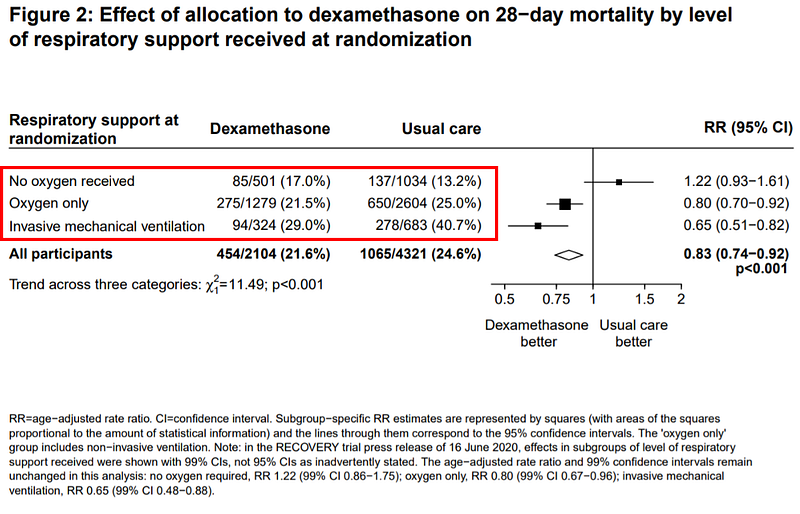
From figure 2 below, dexamethasone lowers the death rate in those requiring respiratory support of supplemental oxygen (by 20%: from 25% to 21.5%) or mechanical ventilation (by 35%: from 40.7% to 21.6%). These are in comparison to the usual care, and results are statistically significant.
As they wrote: “Dexamethasone reduced 28-day mortality by 35% in patients receiving invasive mechanical ventilation (rate ratio 0.65 [95% CI 0.51 to 0.82]; p<0.001) and by 20% in patients receiving oxygen without invasive mechanical ventilation (rate ratio 0.80 [95% CI 0.70 to 0.92]; p=0.002).”
But in those needing no oxygen support, dexamethasone had no effects on Covid-19 mortality rate (p = 0.14; CI 0.93 to 1.61). If the p-value exceeds 0.05 and the confidence interval (CI) range includes one, it means results are not statistically significant and due to chance.
“No benefit was demonstrated in hospitalised Covid-19 patients who were not receiving respiratory support and the results are consistent with possible harm in this group,” the authors wrote. It is a “possible harm” because 17% of the dexamethasone group died compared to 13.2% of the usual care group, but this result is non-significant.
2. 28-day Mortality by Baseline Characteristics
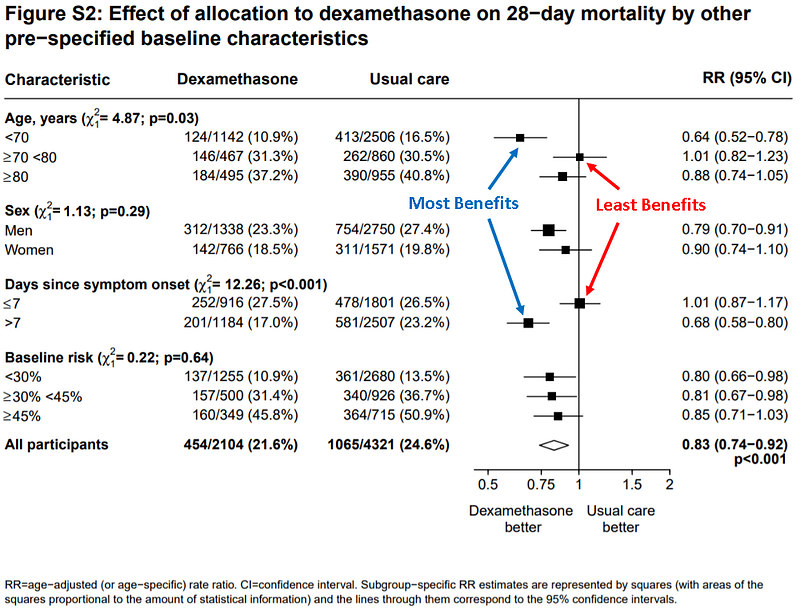
From the supplementary figure 2 below, they also investigated what type of people would benefit most from dexamethasone’s life-saving effects. To this end, they separated their analyses by age, sex, days since symptom onset, and baseline risk factors (e.g., comorbidities).
Relative risk is one (i.e., represented by the vertical line) indicates no differences in efficacy between dexamethasone and usual care. Following this, it appears that dexamethasone did not help those aged between 70–80 years and those with more recent symptom onset (i.e., <7 days). In contrast, dexamethasone had the greatest benefits on those aged <70 years and those having late symptom onset (i.e., >7 days), as evidenced by the black square furthest away from the vertical line.
3. Hospital Stay and the Need for Ventilators
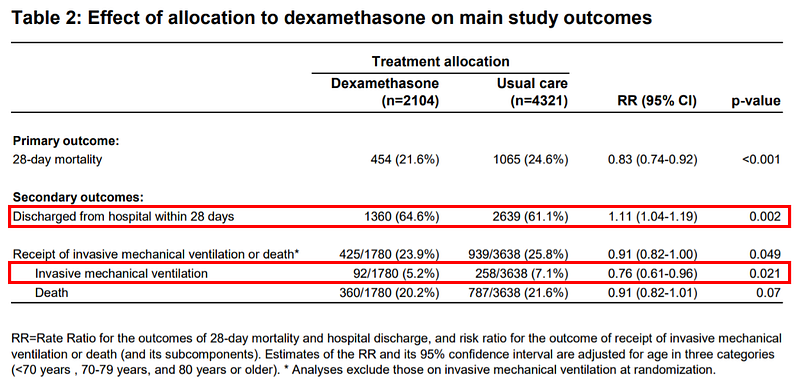
Other results they obtained are in Table 2 secondary outcomes. Dexamethasone treatment increased the likelihood of being discharged from the hospital within 28 days (from 61.6% to 64.6%) and decreased the possibility of requiring mechanical ventilation later on (from 7.1% to 5.2%).
KEY POINTS
Methods of the Oxford RECOVERY trial are robust with the only slight drawback being an open-label design. Covid-19 patients are appropriately randomised into dexamethasone or the usual care group. This is evidenced by the similar baseline patients’ characteristics between the two groups in terms of age, sex, comorbidities, etc.
“The RECOVERY trial provides clear evidence that treatment with dexamethasone 6 mg once daily for up to 10 days reduces 28-day mortality in patients with COVID-19 who are receiving respiratory support,” the authors wrote. “Based on these results, 1 death would be prevented by treatment of around 8 patients requiring invasive mechanical ventilation or around 25 patients requiring oxygen.”
Dexamethasone did not help patients that did not need respiratory support. As their pre-print added: “There was no benefit (and the possibility of harm) among patients who did not require oxygen.” The harm is only a possibility because, as mentioned above, this result did not reach statistical significance.
Is there any fault that would undermine the breakthrough findings of the RECOVERY trial? At least I, just as a postgraduate student, could not find any.