
How to Beat Depression With Exercise
Rewriting the narrative of mood disorders through personal journey and research

A few months ago, the media enthused over a study about exercise as the best anti-depressant [1]. The headlines read like this in The Guardian:
“Exercise is even more effective than counselling or medication for depression”
In this post’s three sections, I’ll introduce you to three contradictory facts: first, why I don’t trust the data that fueled those headlines; second, how exercise affects the biological underpinnings of depression; and third, how you can exploit this knowledge to make that headline true for yourself after all.
Before we get to that, I’ll let you in on
My brush with depression
For a couple of months last year, I was mentally and emotionally in a very dark place. Had I seen a shrink, I would not have qualified for the full depression diagnosis.
I didn’t check all the diagnostic boxes. But I was pretty close. Years of no reward for all the work I had put into my business, compounded by financial constraints, had driven me there. On top of that, I find it very difficult to open up to anyone about such problems.
I fully subscribe to what Pablo Escobar said:
“No point talking about your problems. 80% of the people aren’t interested, and the other 20% are happy you have them.”
My wife was the only one who knew about me being in that dark place. But I got out of it. Partly because I’m a student of Zen and partly because I’m a scientist. As the latter, I learned how to find the instruction manual for my mental health in Mankind’s Library of Medicine. And I knew where to look.
Since pills were out of the question for me, I decided to check the evidence for exercise. After all, exercise is medicine. So, let me take you with me on my journey of discovery.
How to trust the evidence
Barely a year ago, researchers from the University of South Australia (UniSA) published the results of an umbrella review of the
“ Effectiveness of physical activity interventions for improving depression, anxiety and distress" [1]
For the uninitiated, an umbrella review is a review of reviews. Reviews collate the results of many trials that independent research groups conducted to answer the same or similar questions.
The idea is to get a more solid understanding of the balance between the benefits and harms of interventions. After all, individual trials often lead to conflicting results and conclusions. That’s what makes summary reviews so attractive. And that’s why we are faced with an exponential increase in reviews but also with an exponential decrease in review quality and usability.
Researchers from the Meta-Research Innovation Center at Stanford University (METRICS) estimated that only around 3% of reviews are of good quality and clinically useful [2]:
“An evaluation of the landscape of current systematic reviews and meta-analyses suggests that … only about 3% of them are both well done and clinically useful”.
What if the useless ones make it into an umbrella review? I believe you recognize this as a rhetorical question.
So, my first step was to check the quality of the reviews that made it under the UniSA umbrella. As for almost anything in medicine, there exist guidelines on how to conduct umbrella reviews [3] and how to judge the quality of their component reviews [4].
The latter guideline’s AMSTAR 16-item quality scoring grades reviews as having a "high," "moderate," "low," or “critically low” value. Of the 97 reviews that made it into the UniSA umbrella review, 77 (79%) had the lowest grade (critically low), and only 10 scored as “high” quality.
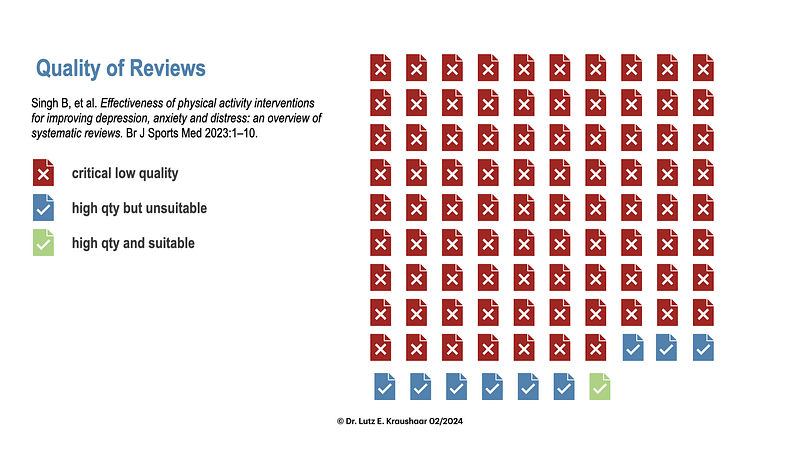
Of those ten, only one compared exercise with pharmacotherapy in depression patients [5]. Of the remaining nine, only one used depression patients as subjects; the other eight only measured degrees of depressive symptoms as outcome variables in different patient groups and always compared to no intervention.
That’s not my evaluation, mind you; it’s what the UniSA researchers themselves observed. To find out, you only need to dive into their paper’s supplementary material.
So, of the 97 studies, only one ticked all the right boxes: high quality (or rather, not “critically low”), depression patients as subjects, and comparison with pharmacotherapy.
And what did it say?
“When compared to psychological or pharmacological therapies, exercise appears to be no more effective, though this conclusion is based on a few small trials”.
And compared to no intervention?
“Exercise is moderately more effective than a control intervention for reducing symptoms of depression, but analysis of methodologically robust trials only shows a smaller effect in favour of exercise”.
Moderately more is not 1.5 times.
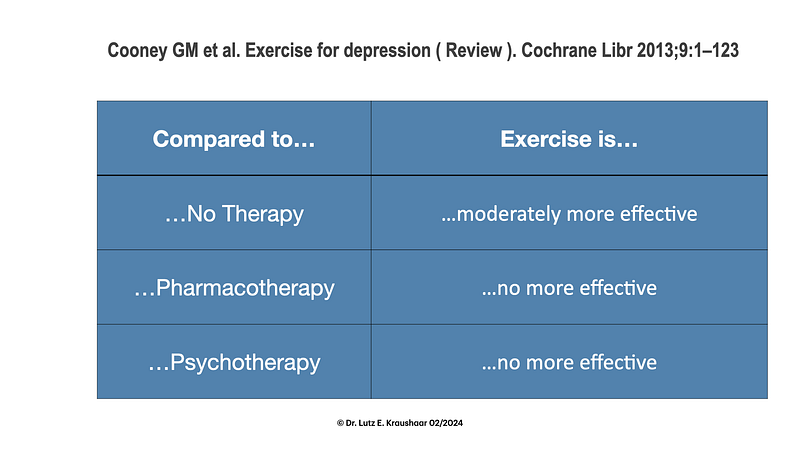
Not coincidentally, this was a Cochrane review. The Cochrane database of systematic reviews is the undisputed and unparalleled white knight of this research genre. Just check out their guidelines for what it takes for your review to be admitted to the Camelot of reviews.
Now you understand my skepticism about the media-savvy headlines.
Does that destroy our hope for the beneficial effects of exercise on depression?
No, I didn’t think so.
What the umbrella review shows is an absence of credible evidence. And that’s not the same as evidence of the absence of an effect.
So, in the next section, we shall look at the biological pathways to depression. Once we understand them, we can check whether and how exercise affects them.
The biological underpinnings of depression
When trying to understand depression, the questions of what is mood and what are emotions come up. Their closest physical representations are the patterns of neuronal activities in the brain. Their central elements are the synapses, those structures where one neuron air-kisses another.
Into this cleft between two neurons, one spills its neurotransmitter molecules, which stimulate the receptors of the other. That stimulus then excites the second neuron or puts it to sleep, so to speak.
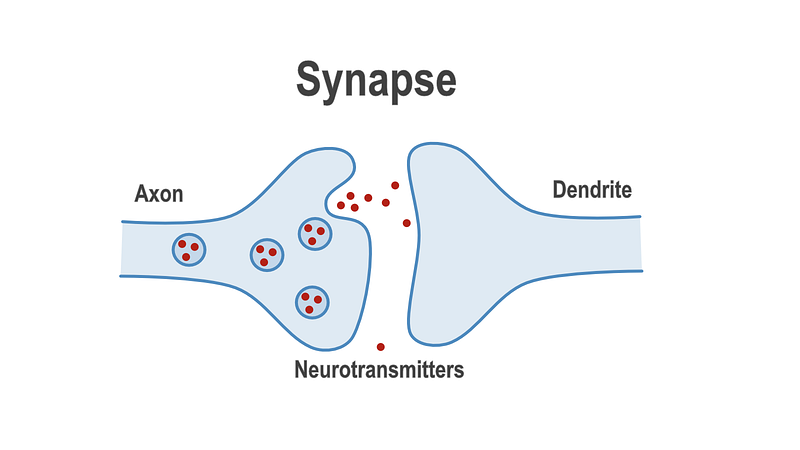
No one disputes the fact that our emotions emerge from the hypercomplex patterns of this synaptic activity [6]. That’s why a lot of research has gone into figuring out the role of the neurotransmitters and other potential culprit actors on the synaptic stage.
The first-generation suspects — monoamines
You have probably come across the names of this triumvirate: serotonin, dopamine, and noradrenaline. A lack of those predisposes to depression. That was, in essence, the monoamine theory of depression. It sounded logical because drugs that potentiated their activity reduced depressive symptoms. The only problem with this is that while the drugs’ potentiating effects are immediate, the reduction in depressive symptoms is not. It typically takes several weeks before depression improves noticeably. And a sizeable proportion of depression patients fail to respond to them. So, for our purpose, we want to keep monoamines on our radar, but we need to look out for other potential points of attack.
GABA and glutamate
Gamma-aminobutyric acid (GABA) is the brain’s chief inhibitory neurotransmitter with a calming effect. There are noticeable deficits of GABA and glutamate in certain brain regions of depression patients. Ketamine, a drug that very quickly increases the levels of GABA and glutamate, also acts very fast on depressive symptoms. So, here we have an attractive target for our planned lifestyle interventions.
Neurotrophins
Neurotrophins promote the growth of new neurons. That’s why they are called growth factors. Neurotrophins also help to keep neurons alive and maintain the plasticity of neuronal networks. Brain-derived neurotrophic factor (BDNF) is probably the most prominent member of that family of molecules. Many depression patients show reduced blood levels of BDNF. Since BDNF levels not only increase after anti-depressant treatments but also correlate with improved cognitive performance (in depression patients and non-patients), we ideally want to nurture that molecule through our lifestyle interventions.
Inflammation
Inflammation is an essential mechanism for removing damaged cells, tissue repair, and many other housekeeping processes. However, if inflammation becomes chronic, it can promote the onset of clinical depression.
Chronic inflammation is the backdrop to long-standing infections (think COVID), cancer, auto-immune diseases, and aging. The latter has received its own title: inflammaging [7]. A correlation between depression and a heightened state of inflammation has been shown in many studies.
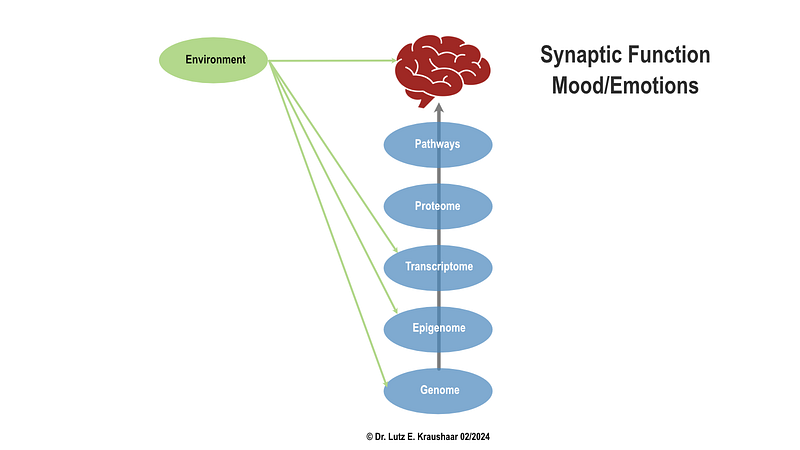
However, not everyone who has high levels of inflammation falls into depression, and not every depression patient has elevated inflammation levels. Similarly, not all patients show the same neurobiological profiles that I have mentioned above. There is far more to depression and synaptic activity than these pathways, and there are also others that I haven’t described. If any one of those pathways was the singular cause of most cases of depression, we would know by now.
This situation is typical for highly complex interactions between different pathways that will play out differently in different people. That makes prediction and treatment a bit of a game of chance.
So, the best we can do to increase our chances of winning this game is to knock out as many of depression’s potential points of attack as we can.
As you will see in the next section, exercise plays a very prominent role in that strategy.
Exercise has effects on the depression pathways.
Exercise and monoamines
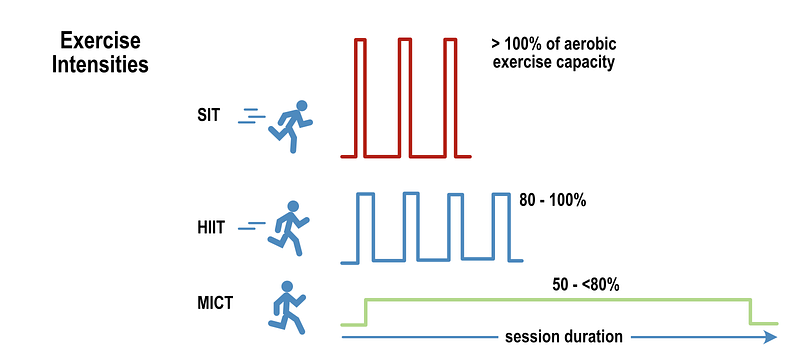
Exercise stimulates the release and function of all three monoamines [8]. The magnitude of monoamine release depends very much on the intensity and duration of exercise. Your best bet at triggering a noteworthy monoamine response is to exercise at intensities of at least 50% to 80% of your maximal oxygen uptake capacity (Vo2max) [9]. These insights come from studies of continuous exercise modes.
If intensity is the trigger, then high-intensity interval training (HIIT) and sprint interval training (SIT) should do the trick, too. The advantage of HIIT and SIT is a remarkably lower time commitment, as I have explained in another post and also here.
Exercise and GABA
There are only a few studies on the long-term effects of exercise on GABA levels in the brain. The limited evidence that we have points to an increase in GABA in response to higher-intensity exercise [10].
Interestingly, a novel finding is that exercise stimulates GABA-receptor activity in the brain [11]. That is, even without increasing GABA itself, the upregulated receptor activity would potentiate its effects. ‘Do more with less’ seems to be a principle invented by Mother Nature.
Exercise and BDNF
A recent review concluded that high-intensity, but not low-intensity, exercise increases BDNF levels in young adults [12]. When you dig deeper, it’s difficult to make sense of the results. Increases, decreases, and no changes have been reported for all sorts of exercises, from high-intensity interval, functional, or power training to lower-intensity routines [13].
One reason is that BDNF measurements are often incompatible between studies. If one study measures BDNF in blood serum and the other in plasma, concentrations differ by up to two orders of magnitude [14]. To complicate matters further, BDNF can easily switch between serum and plasma.
But all in all, the evidence suggests that acute exercise of higher intensity triggers transient increases in BDNF, with blood concentrations returning to pre-exercise levels within an hour or so [14]. That means the frequency of exercise plays a role in activating the BDNF-depression axis on top of intensity.
Exercise and inflammation
What interests us here is the effect of exercise on inflammation biomarkers in patients with chronic inflammation.
A recent systematic review concluded that both aerobic and strength training dial down the inflammatory state [15] not only by reducing its biomarkers but also by increasing anti-inflammatory markers such as adiponectin. The review’s component trials did not allow us to identify which exercise intensity is best.
Another review delivered a clearer answer to this question: while all exercise interventions reduced chronic inflammation, middle-aged adults did better with higher-intensity exercise [16].
The take-home points for exercise
- Exercise has a positive effect on all known major pathways of depression
- To elicit a positive effect, an exercise intensity above the aerobic threshold is probably best
How do you know whether your exercise brings you across that critical threshold of intensity? After all, everybody’s fitness level is different. The answer to that question is “the rate of perceived exertion (RPE). Fortunately, we have a visual scale for that, the OMNI scale of RPE.
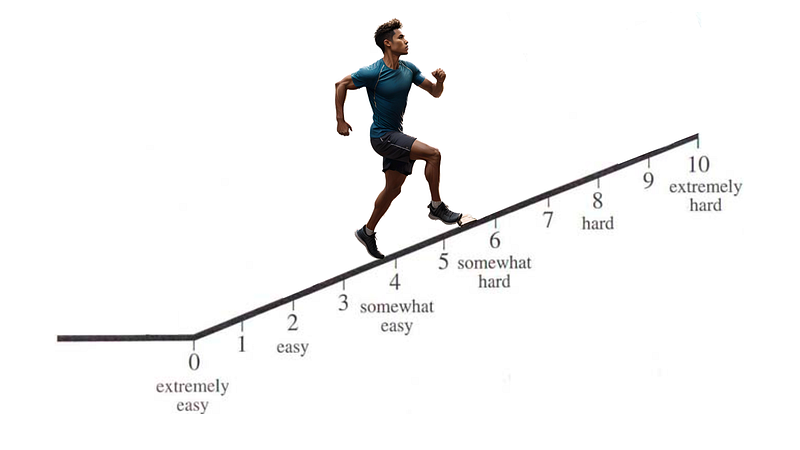
If you would describe your exercise as at least “somewhat hard”, you are in the right zone. “Hard” would be an intensity that you can’t keep up for longer than a few minutes. And “extremely hard” is what makes you stop within 60 seconds. So, get into the zone above level six, and you should be fine.
The search for the anti-depressant exercise prescription
I am, of course, not the only one advocating exercise as a first-line intervention to maintain and restore mental health. The authors of an article in the Annual Review of Medicine came to the same conclusion [17]:
“…aerobic and resistance exercise training hold promise in the treatment and management of mental health conditions, particularly depression and anxiety.”
The purpose of exercise in the context of depression is to elicit an anti-depressant response.
We have seen in the previous sections that such a response is more likely to happen if exercise is of sufficient intensity. And here is where the problem lies for many people with major depression.
When your motivation to do anything at all is in sub-zero territory, exercise is not on your radar. I feel you. I was once pretty close to that stage.
Conclusion: My victory over depression
At the end of my journey through the Library of Medicine, I realized that I was already winning my battle with depression. Having taken the right medicine — exercise– all along had protected me from going down the rabbit hole of depression. I simply had to dial up the intensity a bit.
I exercise every day. I spend 90 minutes in the gym five times a week. 60 minutes of cardio and 30 minutes of strength training. Now I go to the limit every time I train. The reward is a state of post-exercise exhaustion cum exhilaration. It reset my emotional dial from minus to plus. Long enough to see me through most days. And ultimately, I left that dark place behind. Entirely.
If you can get yourself to just put on your sneakers and get going, you are already halfway there. Sweat all that emotional load off your chest, and you’ll remember that post-exercise exhilaration long enough to hit repeat the next day.
That’s why I firmly believe that exercise beats antidepressant pharmacotherapy hands down. Whether it’s 1.5 or 5 times better, I couldn’t care less.
Cited References
[1] Singh B, et al. Br J Sports Med 2023;
[2] Møller MH, et al. Intensive Care Med 2018;
[3] Choi GJ, et al. J Lipid Atheroscler 2023;
[5] Cooney GM, et al. Cochrane Libr 2013;
[6] Fries GR, et al. Mol Psychiatry 2023;
[7] Fülöp T, et al. Gerontology 2019;
[8] Lin TW, et al. Brain Sci 2013;
[9] Kruk J, et al. Free Radic Res 2020;
[10] Ren J, Xiao H. Life 2023;
[11] Levin O, et al. J Clin Med 2021;
[12] Fernández-Rodríguez R, et al. Sport Heal Sci 2022;
[13] Murawska-Ciałowicz E, et al. Sci Rep 2021;
[14] Walsh JJ, et al. Appl Physiol Nutr Metab 2018;
[15] Tan L, et al. Exp Gerontol 2023;




