
Personal Health
Have You Ever Been Emergently Defibrillated?
Personally, I don’t recommend it

The other day, B. A. Cumberlidge. presented a writing prompt that asked us to recount a day that contains an everlasting memory. While there are plenty of noteworthy days to recount, one story jumped immediately to mind.
It was the day my friend had a heart arrhythmia on Blackcomb Mountain in British Columbia and had to be helicoptered off the mountain to the Whistler Clinic. It was quite a day.
However, it would be a little disingenuous to tell that story without also admitting that something similar happened to me — but without the helicopter ride. My story is a bit tamer, but with one dramatic similarity — getting shocked by a defibrillator.
My friend’s story happened a few years before mine, but the fact that we both had the same medical procedure done at the clinic at Whistler makes for mildly comedic coincidence.

I am going to conveniently blame the genesis of my story on some other friends. See, on this occasion, a couple of other firefighter friends and I had gone up to Whistler to ski and, of course, party it up a little.
This was a pre-cursor to my family coming up a few days later and spending the rest of the week up there. A few days of wild party, a few days of bucolic family bliss.
Friends leave, family shows up and we enjoy a quiet evening in the condo. It was early December and the skiing was okay, but not necessarily epic. So, the next day we woke up and were deciding whether to make it a ski day or not based on weather. I noticed in the morning that my chest felt a little funny.
It wasn’t a pain, but sort of a feeling like I needed to take a deep breath, however a taking a deep breath didn’t relieve the sensation. I felt my pulse and it was fast. I counted it at about 150 beats per minute.
That’s a fast rate for someone that isn’t engaged in exercise, but not an acutely dangerous rate for someone in reasonably decent shape with no cardiac history, like me. So, I just sort of waited it out; hoping it would just go away.
We whiled away time in the condo, watched a movie, had lunch etc. I didn’t feel bad, just different, and I knew it was abnormal for my heart rate to be so high.
Finally, I gave in and admitted that I should try and figure out what was going on. I considered going to the fire station, as it was right across the street from our condo, and that is what I would have done at home. In Washington, most all the fire departments do their own Emergency Medical Services (EMS), meaning they have EMTs and paramedics — and most importantly, cardiac monitors.
At home the firefighters at the local station could just hook me up to the monitor and take a look. No such luck in British Columbia as the EMS service is done by a Provincial third service agency. So, I had to hoof it to the clinic.
I checked in, gave them a credit card since my U.S. insurance wasn’t going to cover things up front and told them that the reason I was there was for an elevated heart rate.
Being medical professionals, they met that with all the cold skepticism I would have applied if I was in their shoes. It was interesting being on the other side of the medical care delivery dance.
So, when the tech came out and put an SpO2 monitor on my finger she proclaimed: “You have a really high heart rate.” WHHHAAAAAT? No way! (I said that sarcastic part silently to myself.)
They hustled me back pretty quickly after that. The next fun part was when I asked the tech to see the EKG. I did have enough of my sense of humor to at least consider holding it upside down, scrunching up my eyebrows and saying, “looks like squiggles”.
But I think that is what she expected me to do, and I had not yet admitted that I was a paramedic. In fact, I am pretty sure not very many people ask to see the EKG. But she relented and I could see right away it was Atrial Flutter with a 2:1 AV block.
Huh, I guess that explains it.
I also had a pretty good idea of what their plan of attack was going to be to fix me up. Some “electrical therapy” was imminent.
Soon, the physician and a nurse were involved. The physician came over to explain what was going on. She was really nice, and I shared that I was a paramedic and that I had a pretty good handle on the course of action.
Later on, when I had recurrent bouts of A-Flutter and before it was permanently treated, my episodes would have variable heart rates and often be slower and more tolerable. That first time, though, it had remained at 150 all day and showed no signs of doing anything different. Common practice is to attempt to convert newly presenting Atrial Flutter rather than controlling the rate with drugs.
We discussed how that was really the only treatment appropriate for the setting, especially since a major hospital was nearly two hours away in Vancouver. So, the nurse put in an IV and gave me some fentanyl and versed for the upcoming procedure.
The next fun part was when the nurse (now aware that I was a paramedic and had done emergent cardioversion in the field numerous times) asked me how best to put on the defibrillation pads.
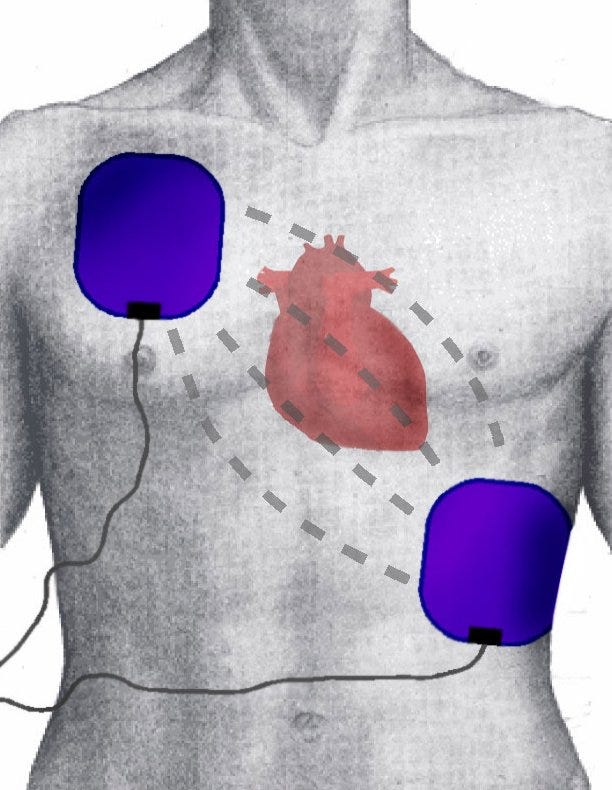
These days there is no grabbing of paddles for this event, rather large sticky pads are applied to the patient and the current is delivered through them.
I suggested Anterior-Posterior (AP) placement as I figured shorter distance was better (medically either AP or lateral placement is appropriate), and I made sure they had really good adhesion to my skin. I knew it would hurt, but I figured I might as well do everything I can to minimize it. After all, I had a significant vested interest in the procedure!
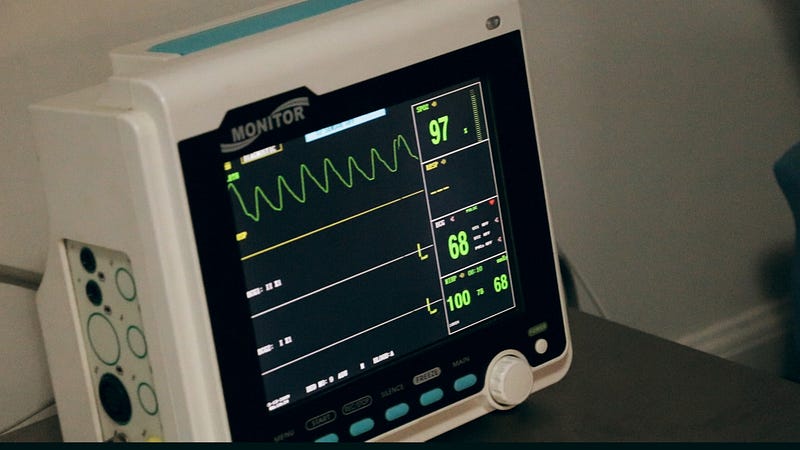
For your viewing pleasure, below is a video I found on YouTube that mimics the procedure I had done. There are some small differences. Being a small regional clinic, there was no cardiologist present — he was consulted by telephone in Vancouver; also, no large team of nurses, just the one plus the doctor.
Also, the video is labeled as a cardioversion of A-Flutter, although you can see from the monitor that she is probably actually in Atrial Fibrillation, not Flutter. Minor difference though, as the therapy is the same. Plus, and most importantly to me, she was given Propofol, which does a much better job of knocking the patient out.
You can see that she is pretty sedate, and they actually give her oxygen because her SpO2 drops after they snow her. She doesn’t even know what happened or feel anything. I was definitely awake before, during and after!
Back to my experience:
After the medication was given and the pads placed, the doctor came in and started messing around over by the defibrillator. I appreciate that she knew that I knew what was going on. She attempted to do one of those, “let’s do this at the count of three” type things while knowing all along that she was going to hit the button on one.
But, even with the volume low, the sound of the defibrillator charging is unmistakably distinctive.
It hurt. I am not going to lie. And I remember all of it, in spite of the Versed which can have a retrograde amnesiac effect on some. Not me, apparently.
But both of those drugs wear off rather quickly, and with my heart now ticking along at a nice leisurely 60 BPM in a normal sinus rhythm it was only 45 minutes or so before I was headed back to the condo to enjoy the rest of our vacation.
If you want to hear the rest of the story, here is my recounting of how a cardiologist burned the area around my heart valve to permanently prevent the Atrial Flutter:
If you liked this article, you may also like:
Timothy Key spent over 26 years in the fire service as a firefighter/paramedic and various fire chief management roles. He firmly believes that bad managers destroy more than companies, and good managers create a passion that is contagious. Compassion, grace and gratitude drive the world; or at least they should. Follow me on Instagram, Facebook, and Twitter, and join the mail list.






{kind=link}