
Emergence from COVID-19
How Testing Can Open the Doors for Rebirth of Community

COVID-19, the life-threatening disease caused by SARS-COV-2 virus, is frightening. I bet that most readers feel lost in all the talk of testing, deaths, social distancing, personal protective equipment, and all the pronouncements coming from various government officials and news reports. There are a lot of unknowns, but there are ways to mitigate the unknown.
We all have those nagging questions, even if we suppress them, relegating them to our subconscious. Do I have it? Can I go to work? Who has it? Who will give it to me? And will I DIE??? Testing is key. Widespread testing — See my previous article that dealt with screening tests. These tests would have been most useful in the early days of the pandemic or local epidemic. But the virus and its illness are now spreading rapidly. We need to look at other types of testing, and that will give us genuine hope in this time of global despair.
I have been frightened and confused, too. I am in the high-risk group, being in my 70s. But we can and should look at the overall picture. We should analyze where we are, where we need to go and what we need to do. We need to do everything we can to limit the death toll, and the chronic pulmonary disease that is sure to hit those who survive severe COVID-19.
I think there is a logical way to look at this disease, even in the fury of its assault. But it will require massive testing, something our government seems to ignore. I know from inside sources that testing in upstate New York is very limited. I am sure the same is true all over the country. We are way behind. But if we need more testing, we need to be clear about what kind of testing. I will look at what tests are available and how to apply them for benefit of each individual as well as populations. The perspectives are different. Both are necessary.
Our governmental leaders appear on TV talking about the issues they see. People like Dr. Anthony Fauci and Dr. Deborah Birx tell us what the government is doing to manage the spread in the population as a whole. It does not matter at this point whether we agree or disagree with them. The point is this: their role is to manage populations, or sizeable groups, of us the people. That is a vital part of what we must do. But it is not their job, nor their expertise, to look at any individual and say what that single person should do. I think there is more we could, and should, be talking about. The rest of this article looks at my views on how to truly manage this viral assault on humanity, from a population to a more individualized perspective.
One thing we need to keep in mind. COVID-19 causes a protracted series of events in those who have moderate to severe symptoms. COVID-19 has been around for 3 months now, but only a small percentage of people officially counted as infected have recovered. The rapid spread of SARS-COV-2 virus across Europe and the United States suggests to me that there is a lot of transmission from asymptomatic, infected people to the uninfected. We just do not have any numbers about the asymptomatic population, nor about the minimally symptomatic population.
Let’s look at the various groups within the general population. Then I will describe the various types of tests and their role. I will also focus on the asymptomatic population and how we can use testing to begin to safely allow us to once again mingle freely without fear. Ultimately, vaccination is the ultimate safety valve, but that is a long way off. In the meantime, there is a logical way to enable at least some of us to venture out into our dangerous world. All we need is wide spread testing to find out who is and who is not infected, and who and who has not been infected in the past. These steps can be achieved if our government and business and health care workers expand testing.
COVID-19, the life-threatening disease caused by SARS-COV-2 virus, is frightening. I bet that most readers feel lost in all the talk of testing, deaths, social distancing, personal protective equipment, and all the pronouncements coming from various government officials and news reports. There are a lot of unknowns, but there are ways to mitigate the unknown.
We all have those nagging questions, even if we suppress them, relegating them to our subconscious. Do I have it? Can I go to work? Who has it? Who will give it to me? And will I DIE??? Testing is key. Widespread testing — See previous article. But we need to look at the types of testing, and that will give us genuine hope in this time of global despair.
I have been frightened and confused, too. I am in the high-risk group, being in my 70s. But we can and should look at the overall picture. We should analyze where we are, where we need to go and what we need to do. We need to do everything we can to limit the death toll, and the chronic pulmonary disease that is sure to hit those who survive severe COVID-19.
I think there is a logical way to look at this disease, even in the fury of its assault. But it will require massive testing, something our government seems to ignore. I know from inside sources that testing in upstate New York is very limited. I am sure the same is true all over the country. We are way behind. But if we need more testing, we need to be clear about what kind of testing. I will look at what tests we need and how to apply them for benefit of each individual as well as populations. The perspectives are different. Both are necessary.
Our governmental leaders appear on TV talking about the issues they see. People like Dr. Anthony Fauci and Dr. Birx are telling us what the government is doing to manage the spread in the population as a whole. It does not matter at this point whether we agree or disagree with them. The point is this: their role is to manage populations, or sizeable groups, of us the people. That is a vital part of what we must do, but it is not their job, nor their expertise to look at any individual and say what that single person should do. I think there is more they could, and should, be talking about. The rest of this article looks at my views on how to truly manage this viral assault on humanity, from a population to a more individualized perspective.
One thing we need to keep in mind. COVID-19 causes a protracted series of events in those who have moderate to severe symptoms. COVID-19 has been around for 3 months now, but only a small percentage of people officially counted as infected have recovered. The rapid spread of SARS-COV-2 virus across Europe and the United States suggests to me that there is a lot of transmission from asymptomatic, infected people to the uninfected. We just do not have any numbers about the asymptomatic population, nor about the minimally symptomatic population.
Let’s look at the various groups within the general population. Then I will describe the various types of tests and their role. I will also focus on the asymptomatic population and how we can use testing to begin to safely allow us to once again mingle freely without fear. Ultimately, vaccination is the ultimate safety valve, but that is a long way off. In the meantime, there is a logical way to enable at least some of us to venture out into our dangerous world. All we need is wide spread testing to find out who is and who is not infected, and who and who has not been infected in the past. These steps can be achieved if our government and business and health care workers expand testing.
Testing in the General population.
Thanksgiving day, 2019. No one in the world had COVID-19. No one even thought about it. Since then, the world population has been divided into several groups based on their SARS-COV-2 status. Remember, SARS-COV-2 is the virus. COVID-19 is the disease caused by SARS-COV-2. Here is a diagram of where we have been for the past couple of weeks. Testing to date has referred to screening people for SARS-COV-2 virus. In general, the testing has been limited to people who have symptoms, or for first line care givers. There are a few others who have risk factors that may be tested. But let’s assume that testing is widely available. Here is the scheme:
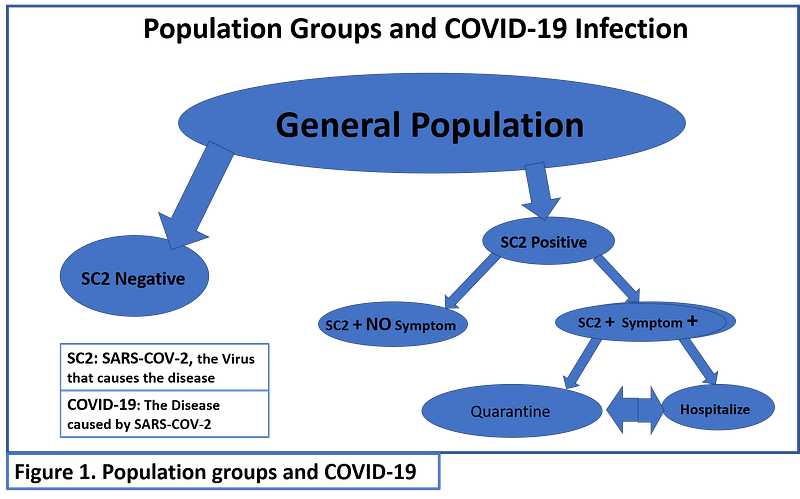
When the COVID-19 Pandemic first hit the United States, there were small numbers of people with active virus. At that time, testing would have been able to show us who was infected, and who needed medical attention. It would also show us who needed protection from measures such as social distancing, or even protective quarantine. But there was a problem. Testing was not readily available. Figure 1 shows the breakdown of the various groups involved in the early days of COVID-19-USA.
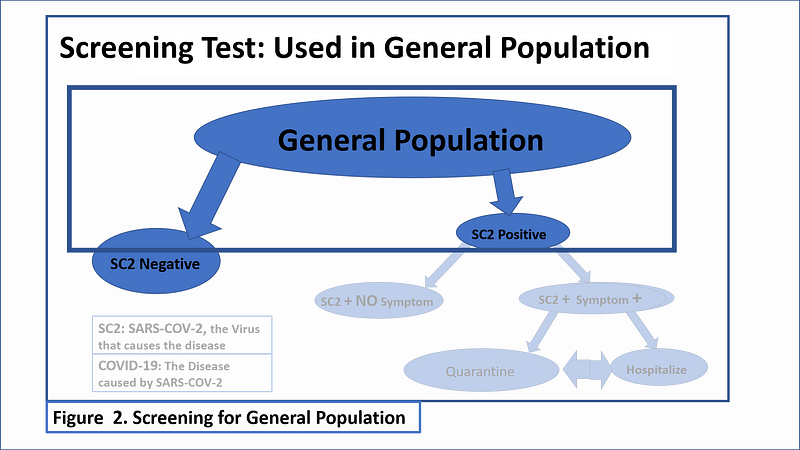
At the outset, we needed screening tests to tell us the answer to one simple question. Did the person being tested have the virus or not? We needed a simple “Screening Test.” We had no such test, but they are just beginning to come onto the market. Hopefully the FDA and CDC will allow these screening tests to be used.
Figure 2 highlights the use of a screening test applied to the general population.
Research Testing for Virus.
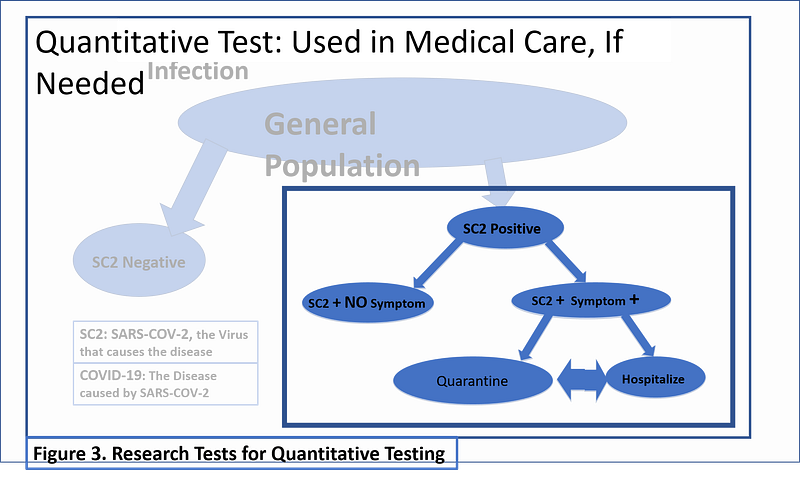
To make matters worse, the testing procedures that were available were for quantitative testing to tell us how many virus copies were present in a given quantity of fluid or tissue. Both screening and quantitative testing uses Polymerase Chain Reaction, or PCR, techniques. The quantitative testing is useful in research. It is also useful in some clinical situations. For example, quantitative PCR tells us how many HIV viruses, or how many Hepatitis C viruses are present in a person’s blood. In active disease, the viral count can be as high as 300,000 virus particle per cubic centimeter of blood. With treatment, the quantity goes down.
Quantitative PCR is of little, if any, use in the clinical management of COVID-19. People with COVID-19 are seriously ill and clinical parameters guide the management. Quantitative PCR may be of academic interest in defining the nature of COVID-19. Once someone is determined to have the SARS-COV-2 virus, screening tests are again used at the end of the illness to document that virus is no longer present. If someone has a negative test, be it screening or more complicated, on 2 successive days, they are considered to be recovered. Figure 3 focuses on the population that needs clinical management and then screening tests when they get better:
The Asymptomatic Population in the Age of COVID-19.
First there is the bulk of the general population who do not have COVID-19, and still have not been exposed to SARS-COV-2. We who are in this group have no defenses against SARS-COV-2. We are at risk for infection and serious disease. When the virus hits us, it can go full force because we have no immunity in the form of antibodies.
Fast forward to today. COVID 19 has gone viral. Headlines are blaring the problems of many cities. No ventilators. No PPE. Medical staff are dying. There are not enough hospital beds. These issues need immediate action. But there is more that needs to be done to protect those of us who are not infected but very, very vulnerable. Most of us will never get there. I hope and pray none of us do, but some will.
We have three basic sub groups: 1. The uninfected general population; 2. Infected people who are symptomatic; and, 3. Infected people who are asymptomatic. People in group 3 are perhaps the biggest threat to group 1, assuming that quarantines and health care are controlling the symptomatic.
General Population amid COVID-19.
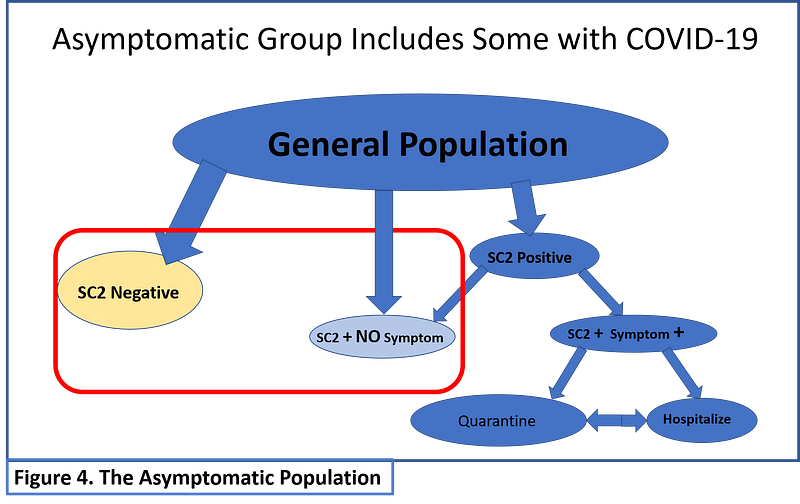
As time goes on, it is clear that the SARS-COV-2 virus is spreading through the general population. I find it hard to believe that there are a lot of people out there coughing and sneezing and spreading this virus. Even with social or physical distancing, people are getting infected in large numbers. Clearly, there are asymptomatic SARS-COV-2 spreaders among us. Figure 4 highlights this group in the red box. The new general population is composed of truly negative people (Yellow ovals), asymptomatic carriers who do not know they have it, and people who may have a false negative screening test for SARS-COV-2.
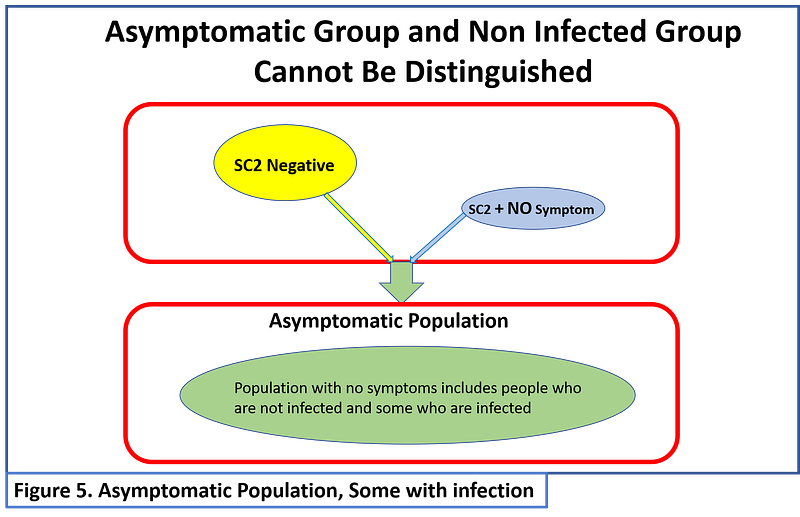
The Mixed Population.
If we mix the uninfected (yellow ovals) and asymptomatic carriers (blue ovals) we can depict this as a green composite group. How do we manage this population? We cannot maintain physical distancing and protective quarantine forever. Eventually, people have to go back to work. We really do need to keep the economy going as much as we can. There are ways to do this with more testing.
Tests for Immunity
A new type of test is needed at this time. We need a test to tell us when someone is immune. At this point in time, these tests are cumbersome and available for only a few people. At least one company, Henry Schein, recently announced that they would begin delivering test equipment to the United States that can test for immunity. When we get an infection, our immune system goes to work. It produces immune globulins, proteins that latch on to the infecting agent, enabling other cells to get rid of the invader. The immune globulins are labeled IgG, The Henry Schein test, and others being developed, measure the presence of IgG that specifically targets SARS-COV-2 virus. If a person has IgG for SARS-COV-2, they are presumed to be immune to the disease. The IgG will prevent it from doing its damage. In general, this is not a new kind of test. It has been refined to measure the IgG that is specific for the virus that causes COVID-19.
Writing for the Washington Post, Paige Winfield Cunningham, has given an excellent summary of the status of these tests.
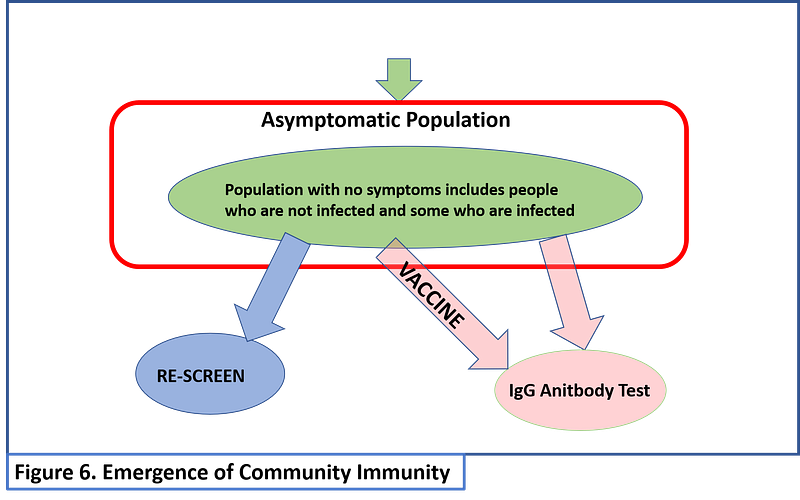
These IgG tests are absolutely necessary to enable us to emerge from our worldwide lock down. People who are immune can mingle freely. They can go to work without getting sick. They can staff InstaCart with no worry. They can work at Amazon warehouses and not get sick. As long as they still practice good hygiene, they cannot pass the disease to someone else. Good hygiene is still mandatory.
For those who are IgG-SARS-COV-2 negative, screening should be done periodically. Furthermore, it would be an excellent idea to have periodic testing for IgG antibody. Were the disease not so deadly, these would not be needed. But for people over 80 years old, exposure to SARS-COV-2 is kind of like playing Russian Roulette with a 6 chamber revolver. For those of us in our 70s, it is like playing Russian Roulette with 2 revolvers with a bullet in only one chamber. Testing of everyone in the country is a bargain compared to the lives ended by needless games of chance.
People who have developed immunity may also help to save others who are really sick. Using a technique called plasmapheresis, the immune globulins are harvested from the person’s blood. The plasma from the donor is then given to the person who is sick. As with blood transfusions, the donor and recipient have to have compatible blood types. This technique has been used for other diseases, including Ebola. Data is inconclusive about effectiveness because of the small numbers, but the treatment seems to be safe with proper precautions.
COVID-19 Can Last for Weeks or Months
Ultimately, we will have a vaccine that will stimulate the body to produce IgG-SARS-COV-2. It cannot come soon enough. Until that day comes, we must rely on innate immunity. Hopefully treatments will evolve that decrease the lethal impact, and the disabling impact, of COVID-19.
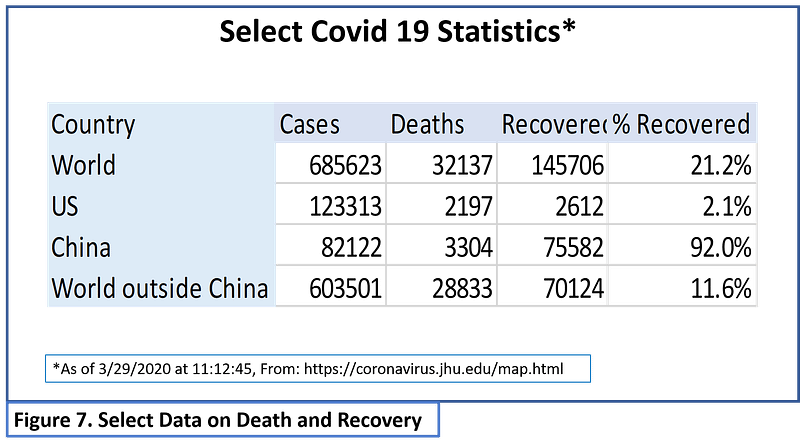
Finally, I want to say a few words about recovery, because no one seems to be talking about that. Recovery from COVID-19 is a very slow process. The Johns Hopkins map that tracks cases, deaths, and recovery shows a significant lag between infection and recovery. Figure 7 shows some select data from 3/29/2020. China, where the disease began, still has several thousand people who have not yet recovered. To date, only a minority of people infected with SARS-COV-2 have recovered. It seems the disease itself can last weeks to months. Furthermore, I have reviewed many CT images of people with COVID-19. These CT scans show significant damage that will probably leave people with chronic respiratory problems for the rest of their lives. The impact of COVID-19 will be around for decades. You can find up to the minute data at this link.
One small piece of good news. I first gathered the data for Figure 7 three days ago. Since then, the percentage of people in the United States who have recovered has increased from 2.1% to 3.7%. That represents a 173% increase in recovery. Unfortunately, total cases have increased 54% and deaths have increased by 86%. Numbers are grim, but we are slowly, very slowly, trending in the right direction.
The Good News at the End.
In closing, there is good news. People are recovering. With appropriate testing, we will see that there are many people who have had a silent infection. They will be able to return to full activity, to the extent that it exists.
With adequate testing, we can objectively manage population control. With appropriate testing we can also give each of us the information we need to manage our lives to the optimize our health and well-being.
Eventually, the majority of people will develop immunity to SARS-COV-2. They will not get the disease. The will not spread the disease, if they practice good hygiene. The small number of people who are not immune will have ready access to screening if they get sick. Treatments will be available. Sadly, some people will still get sick and die, but most of us will be able to safely live a normal life……That is, IF AND ONLY IF we test, test test!
Stay safe in these troubled times. There is hope for the future in these days when despair can take over. A brighter future still needs our universal participation in social distancing till the future gets here.