
Corona Virus: Why We Need a LOT More Screening

Widespread Screening May Save Lives
The “Novel Corona Virus Disease” is here. What does it mean? What can you do? First, this is not an academic scientific article. I am giving you my analysis of the problem and how I would deal with it if I were still in practice. And if I had all the resources I needed.
This disease has no vaccine to give us immunity. No medications will cure it..
Treatment for this disease has two components. Infected individuals need supportive measures. The general population needs measures to control the spread of the disease. This article will discuss the second mode of interventions.
We need some housekeeping regarding terminology. Corona viruses are a family of viruses. Traditional Corona Viruses cause about 40% of the common colds that go around every year. Our immune systems control these viruses with little difficulty. But there are a few more vicious Corona viruses that have caused major outbreaks around the world. There was the SARS outbreak in 2002. SARS stands for Severe Acute Respiratory Syndrome. It originated in civet cats in China. The virus was transmitted to people, and a worldwide outbreak occurred. A novel Corona virus caused SARS. Then in 2012, there was Middle Eastern Respiratory Syndrome, or MERS. A Corona virus that originated in camels caused the MERS outbreak.
A Corona virus that has a genetic profile similar to the first SARS virus is the cause of the current outbreak. It is not identical to the original SARS virus. But it is close enough that the formal name for the corona virus causing today’s outbreak is “SARS-CoV-2.” CoV refers to Corona Virus, and the “2” designates that it is a second distinct corona virus. The term “COVID-19” refers to the disease that is caused by the SARS-CoV-2 virus. It is a short form of Corona Viral Disease that started in 2019.
There is a lot we do not know about the virus and COVID-19. But we know it can be lethal. It is especially deadly for people who are older or have other medical conditions like hypertension, diabetes, cardiovascular disease, etc.
We do not know details about how the virus spreads. Our lack of knowledge is pin part because it is new, but in part because we have not tested enough people to know. There is a desperate need for widely available testing that can rapidly identify the SARS-CoV-2 virus. Without that we will not know if people have active infection, or if they are asymptomatic carriers. Later in this article I will show you why we need widespread, easily accessible screening and diagnostic testing.
The SARS-CoV-2 virus can cause severe symptoms and death. The death rate is estimated at 2% among those who get sick. Some estimates tag the death rate at about 4%. It rises to about 15% for those over 80.
Treatment of populations, rather than individuals, includes measures to limit the spread of the virus from infected people to those not infected. That may be easier said than done. Some people harbor active virus but have no symptoms. These “carriers” can give the disease to others, who may then be asymptomatic carriers or symptomatic patients. Both groups are contagious.
Some Facts About This Disease
In a soon to be published article, two patients had surgery to remove part of their lungs because they had lung cancer. They had no respiratory symptoms at the time of surgery. After surgery they developed symptoms and were diagnosed with COVID-19 caused by the SARS-CoV-2 virus. When the diagnosis was suspected, the pathologists examined the resected lung tissue and found evidence of active COVID-19. Let me emphasize the events: 1. The patients had no symptoms of any respiratory infection. 2. Lung tissue removed to treat lung cancer showed the tumor. It also showed very active COVID-19. 3. Several days after surgery, the patients developed symptoms of the COVID-19 infection that had been there all along. From a medical perspective, that is truly astounding. In all my training in medicine, I was instilled with the scenario that local infections progress to pneumonia. But here we have a pneumonic infective process progressing to a more widespread infection.
One patient got the SARS-CoV-2 virus from another patient in an earlier hospital admission. At the time, the infection of the other patient with SARS-CoV-2 virus at the time was unknown.
The Washington Post ran a recent article about the rapid spread of the SARS-CoV-2 virus among neighbors on Long Island. One contracted the virus when he drove his already infected neighbor to the hospital. The man who drove the care subsequently gave the virus to his own family members, even though he had no symptoms. Once again, we see how easily the virus seems to spread.
Given that the virus is so easily spread among people, I propose that we need readily available testing for SARS-CoV-2. This can be done with nose and throat swabs. But testing is not always positive, so we need frequent, repeat testing. The reasons for this will become clearer with the illustrations below.
Expecting hospitals and doctors to provide all the necessary testing that is unrealistic.
A representative from the Massachusetts General Hospital was interviewed on the NBC Nightly News on March 4th. He said as much. He stated that going to the doctor or hospital for minor symptoms would quickly overwhelm the medical system.
I agree. But we know that people without symptoms can spread SARS-CoV-2. Testing symptomatic people would overwhelm the medical system. Adding asymptomatic people would destroy it.
I propose that testing be readily available for anyone. This could be done through local pharmacies. Other countries have already done this. Rapid, point of contact testing is available in Germany and in South Korea. It could be done here in the United States.
Of course, this approach mandates that people who test positive cooperate, agreeing to voluntary self-quarantine.
Dr. Li Wenliang, Chinese Whistleblower, COVID-19 Fatality
Dr. Li Wenliang was the first doctor to alert the world about the COVID-19 outbreak that was being treated at his hospital in China. He was arrested and interrogated by the police for “Spreading False Rumors.” He was released and returned to work as an ophthalmologist. He treated an afebrile patient. Dr. Li did not use extra precautions, later saying that he was “careless.” The patient later tested positive for SARS-CoV-19. Sometime after treating this asymptomatic patient, Dr. Li developed a cough on January 10th. The next day he was admitted to the hospital as a patient. He underwent repeated testing for SARS-CoV-19, all of which were negative. Negative, until the end of January when a test finally showed the presence of SARS-CoV-19, and he was confirmed as having the disease, COVID-19. He died from the disease abut a week later. Note that he had repeated testing which was generally negative. Dr. Li had repeated tests that were negative for the virus. That seems surprising at first. But two cancer patients described above provide an explanation. Those two patients were asymptomatic. But they still had lung infections. They did not have sore throats.
Testing for SARS-CoV-2 is done using a swab rubbed on the throat and nasal passages. The two cancer patients had no evidence of upper respiratory infections. They still had significant infections in their lungs. They were certainly sick enough to spread the virus. Yet pharyngeal swabs and nasal swabs would not show any virus. There was little or no virus in these areas. It is possible that a blood test would have shown the presence of viral particles.
A Word About Testing
Modern day testing for diseases uses technology called PCR, or Polymerase Chain Reaction. The PCR can identify specific combinations of DNA or RNA, the genetic chemicals in viruses and all living things. The PCR test can be run on any type of bodily material. The PCR test is used by those web sites that tell you where your ancestors lived. It can tell us who committed some crimes. For infections like COVID-19, the laboratory needs a specimen that contains some of the viral particles. Common sources include mucous on the back of the throat or in the nasal passages. PCR testing can also by used on blood or stool. A problem emerges for the SARS-CoV-2 virus and its COVID-19 disease. The infection is sometimes localized in the lungs, and does not spread to the throat or nose. In this situation, screening tests using throat swabs and nasal swabs will be negative, even though the person is infected. There is no way to easily sample the material localized in the lungs.
Testing blood for SARS-CoV-2 virus is feasible, but it is a novel way of testing. The CDC probably would not approve it. PCR testing of blood may become a medical test for symptomatic or high risk asymptomatic people. Doctors must remain open-minded for that to happen. In the meantime, frequent screening remains the frontline approach.
People, The Virus and the Disease
Let’s look at what is involved in this screening and testing. The average American citizen will fit into one of a few categories when it comes to COVID-19 or SARS-CoV-2.
- Uninfected
- Infected–Asymptomatic
- Infected–Mild Symptoms
- Infected–Severe symptoms.
People who are uninfected will not need further discussion. Their test or screening results are negative. But they should still get periodic screening tests. The medical purists will say that this is unreasonable. But it is the only way to be sure they are not asymptomatic carriers. Monthly or biweekly testing should be done on people who are asymptomatic. More frequent testing should be done if they come in contact with someone who might be infected.
From a public health perspective, infected but asymptomatic people are the most serious problem for spread of the disease in the community.
People with mild symptoms may go to their doctor for testing. But they should be able to get point of care screening that does not require going to the doctor. People with symptoms are also most likely to be under some form of quarantine. They are usually advised to stay home from work or school, or take other measures to avoid other people who are asymptomatic. This group should use masks. The mask will help to prevent the spread of viral particles from the patient to others. A mask worn by a healthy person will not prevent air born virus from landing on them. It will not prevent an infection of the healthy person.
Figure 1: Three Groups of People with SARS-CoV-2
Spread of the Virus
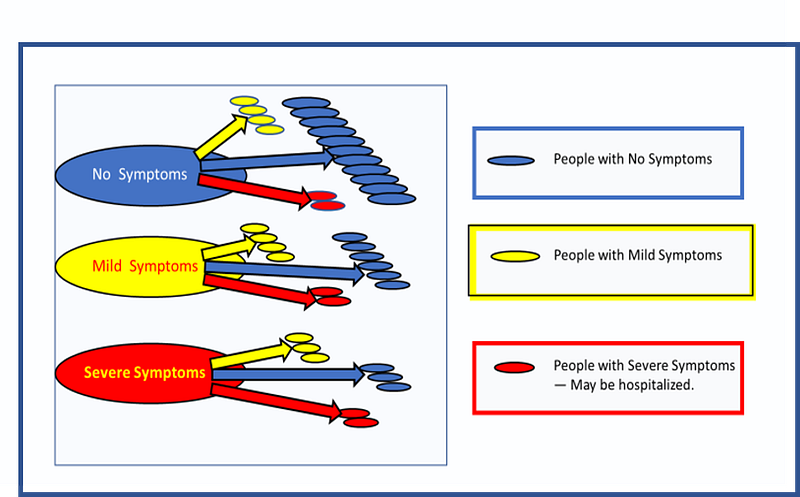
Each group of people with the virus can spread it to others. How common are asymptomatic carriers in the general population? No one really knows. There are no statistics. But their presence creates a risk of deadly outcome, especially in the at-risk groups where extra precautions are warranted.
Figure 2 shows the problem. Blue ovals represent people who carry the virus. They remain asymptomatic carriers. Yellow ovals represent people who develop mild symptoms. Others, shown by red ovals, will develop severe symptoms. People in each group can infect others. Since people with symptoms are more likely to be under some restrictions that limit their contact with other people, they are less likely to infect people in the general population. They will be a significant source for infecting health care workers.
Figure 2: Spread of SARS-CoV-2
Asymptomatic Carriers
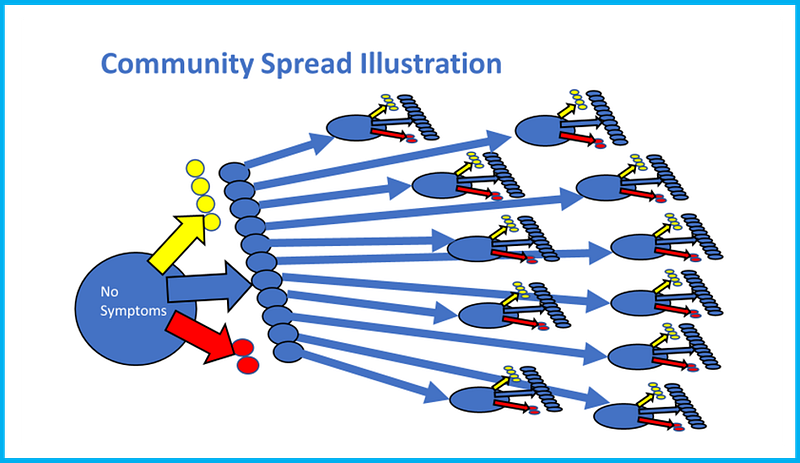
The next diagram shows how the virus can spread among asymptomatic people. I have made up some arbitrary numbers simply to show the concept. The exact numbers for people with SARS-CoV-2 are not known, or at least not publicly available.
The chart assumes there are 17 people. All are infected and contagious. Eleven are completely asymptomatic. Four have mild symptoms. 2 have severe symptoms.
As noted above, I assume that the symptomatic patients are under some form of quarantine. This will limit their ability to infect other people in the general population. Infecting Health care workers who care for them will remain at high risk for infection.
This article is about the rest of us. We are the ones at risk. And look at the chart.
Each of the 11 asymptomatic carriers can spread the virus to produce, for example, 11 other asymptomatic carriers, 4 mildly symptomatic patients and 2 severely symptomatic patients. And so on.
On the diagram, note the visual effect of the wide distribution of the red and yellow ovals.
Figure 3: Spread of SARS-CoV-2 with No Testing
On the next diagram, I emphasize the lack of spread by people who are showing symptoms. I assume that most of these symptomatic patients will undergo some form of quarantine. They will not be able to mingle freely among the uninfected general population.
If the medical quarantine is not effective, the risk for the general population goes up. The asymptomatic people can still spread viral particles. The symptomatic people will spread viral particles as they cough and sneeze. They will contaminate door handles, restaurant or fast food utensils, soda dispensers, goods on shelves of stores they handle and put back, and so on with infective “fomites.”
The virus on these surfaces will remain infective for an hour or more. But for simplicity, let’s maintain the assumption that this symptomatic group is isolated from the general public.
Symptomatic People Enter the Health Care System
Figure 4: Spread of SARS-CoV-2, Focus on Symptomatic Patients
Asymptomatic Carriers Revisited
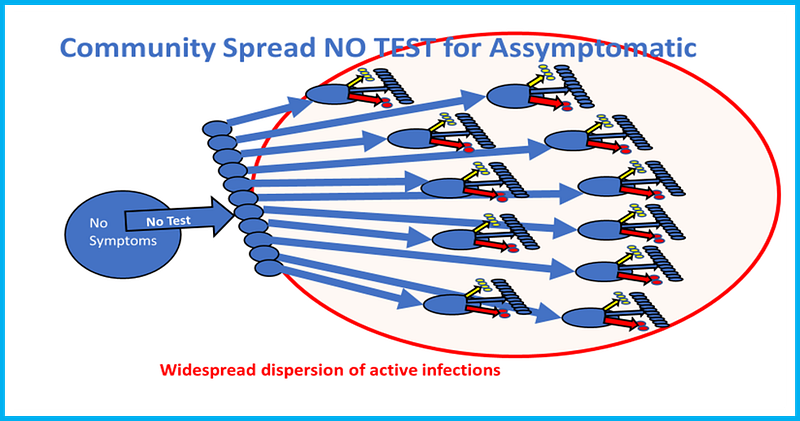
Looking just at the asymptomatic carriers, the next picture again shows the widespread distribution of SARS-CoV-2 infections that occur.
I assume that there is no screening, but the asymptomatic infected person is free to roam among the general public. After all, neither the individual nor anyone else knows that the person is spreading active virus. They have no symptoms.
They have no measurable signs like a fever. No one has done any testing.
Figure 5: Community Spread of SARS-CoV-2 with no testing of Asymptomatic Carriers
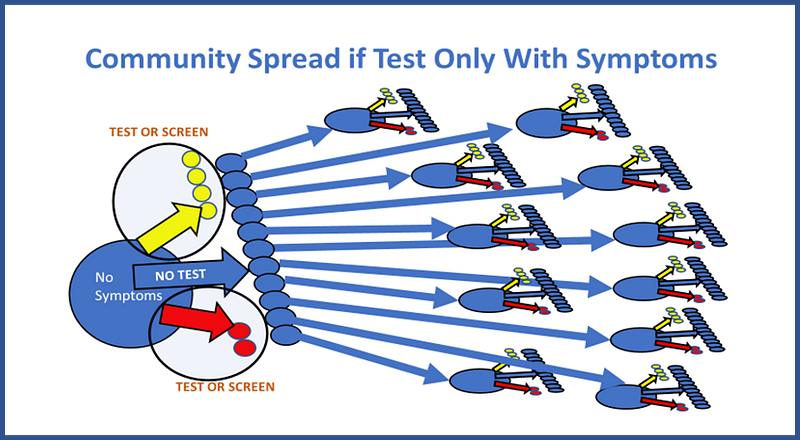
Tests are available around the world for a rapid screen for Corona Virus. Germany and South Korea are two countries that have rapid tests for SARS-CoV-2. Let’s look at these tests. With any test there are 4 possible outcomes.
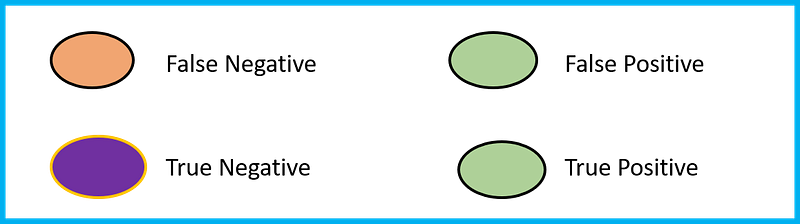
Screening will sort people into 4 different groups
- True Negatives
- True Positives
- False Negatives (Has virus, Screen negative)
- False Positive (Does NOT have the virus, Screen Positive)
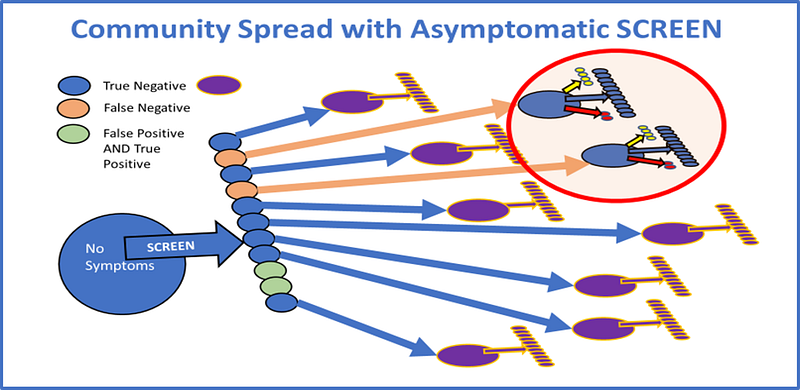
I have now added color coding. Tan represents false negatives. These patients have the disease but screen as if they did not have it. They can still spread the virus to others. These newly infected patients can still spread the virus to others. They may or may not have any symptoms.
True positives (people with SARS-CoV-2 and screen positive) and False positives (people who do NOT have the virus, but tested positive) have green labels. As a result of their test results, they will presumably be under some form of quarantine. They will also need to undergo further testing that will be more definitive. Therefore they are no longer at risk for spreading the virus.
Note, however, the very limited presence of new infections that are symptomatic compared to the “No Test” scenario. Screening., even if it has some false positive or false-negative results, can yield more limited spread of the virus. Doing no testing results in the more rapid and wider spread of the disease.
Frequent widespread screening can have a positive impact. It is also not a once and done intervention. All health care workers must get an annual assessment for exposure to tuberculosis. TB is an occupational hazard. If the PPD tests that turns positive, the presumption is that the person has a TB infection. Yearly screening is sufficient for protection of the health care workers AND their patients.
With SARS-CoV-2, the same concept can be used, except that the screening needs to be done in the general population and it needs to be done repeatedly until the epidemic is fading or a vaccine becomes available.
SCREENING
Screening with pharyngeal and nasal swabs is the primary method of monitoring for SARS-CoV-2 virus. I need to add a couple of new groups with color coding to represent them. First, some people who do not have the disease will test positive. These are known as “False Positives.” They will be represented by green ovals.
Some people who have the disease but test as negative. These are known as “False Negatives.” They represent a serious problem, with high risk of spread of the virus in the community. They will be represented by tan ovals.
Most people who do not have the disease will test as negative. They are known as “True Positives.” They will be represented by purple ovals.
False negative tests have serious implications. They can result in spread of the infection. People who are infected by a falsely negative person can get symptoms, and some may even die. Tests should have a negligible rate of false negative results. People with a “false negative” status are a risk to the community.
False positives in the COVID-19 outbreak have minimal impact. If someone is a “false positive,” they will undergo some kind of quarantine or isolation pending repeat accurate testing. There will be no harmful intervention based on “false positive” status. There will be no surgeries. There will be no toxic medications. There will be some personal inconvenience, but it is a small price to pay for the benefits of testing to find the true positives.
Community Spread With Screening
Figure 6: Community Spread with Screening of Asymptomatic Carriers
Other countries have tested people far more frequent than the United States. In the US, we do not know how widespread the SARS-CoV-2 virus is. We know it has infected people from coast to coast.
A Chinese company claims to have a test that can detect presence or absence of SARS-CoV-2 within 15 minutes.
A US company says it has a product that can give rapid test results. Federal regulations prohibit mass production of these unapproved tests.
The US CDC has already botched its test kit, which had components that did not work. The CDC is the only entity that can produce and distribute tests without special approval from other branches of the government, specifically the FDA.
It is time to unleash American Scientific Enterprise and get some widely distributed tests on the market. We, the people who stand to lose the most, should have access to drive up tests or the equivalent. They are available in other countries.
The CDC does superb scientific work. However, it is too detached from the public to give effective protection to the health and lives of the average American.
Finally, let me say a word about one of the most common steps that public health officials promote: Frequent hand washing.
I agree, BUT…… things are not so simple. I work part time in a large agency with about 175 employees and many more customers. People usually wash their hands in a rest room. In the restroom where I work, people head for the door without washing their hands. All of those “fomites” just got deposited on the door handle. The door opens inward so you have to use the door handle to exit. If the person has some bodily fluid with SARS-CoV-2 on their hand, the door handle is now contaminated and it can remain infective for more than an hour. My approach is simple: wash my hands and then use a paper towel to act as a barrier between me and the fomites living on the door handle. Promoting hand washing is good, but by itself it will be woefully inadequate.
Sadly, the US seems to be backing its way into a serious epidemic of SARS-CoV-2 causing COVID-19. The US is too ill-prepared, and too ill-informed to be effective in preventing the spread of this disease.
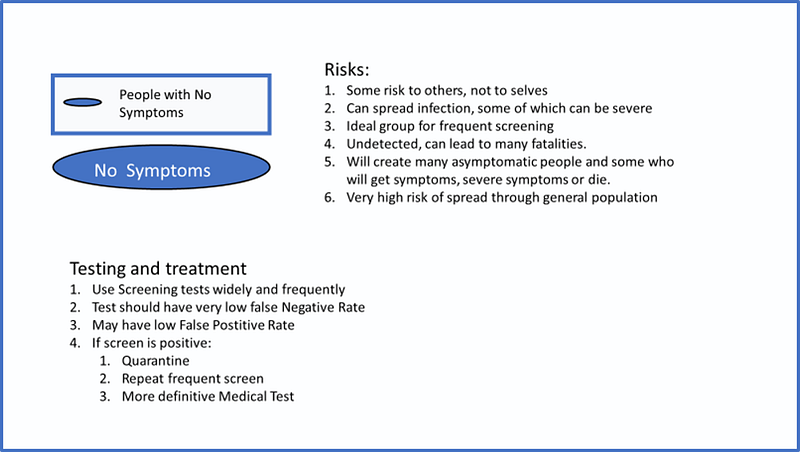
Summary: Asymptomatic Carriers
Figure 7: Summary of Asymptomatic Carrier Issues
Summary: People with Mild Symptoms
Figure 8: Summary of Mildly Symptomatic Patient Issues
Summary: People with Severe Symptoms
Figure 9: Summary of Severely Symptomatic Patient Issues
Conclusion:
The bottom line is simple: Test a lot of people, meaning every one. Test frequently. Quarantine if there is any possibility of exposure to SARS-CoV-2. And until there is an effective vaccine and or treatment.
Right now we cannot do adequate testing. It is time to mobilize America, its private industries, and people. The CDC can do what it is good at: analyze data after the fact.