
Confronting America’s Fixable Depression Crisis
Depression is highly treatable. So why are rates soaring, particularly among young people? We need to acknowledge the scope of the problem, shake the stigma, and embrace solutions known to work, experts say.

This article is part of a Wise & Well Special Report: The United States of Depression.
After suffering a stroke last year, US Senator John Fetterman, a man who’d long seemed sad to those around him, plunged into deep depression. In the pit of his despair, he lost the motivation that had driven him to the pinnacle of politics. He lost weight, stopped showering, and didn’t expect to recover. But with professional help, a mixed bag of remedies and a lot of support from family, friends and even strangers — not to mention an excellent healthcare plan afforded people in Congress — Fetterman pulled back from his self-described brink of existence and got better.
The 53-year-old freshman senator from Pennsylvania joins a growing list of high-profile Americans who’ve been crushed at times by the darkness (tennis phenom Naomi Osaka, gritty Tour de France biker Mark Cavendish, actress Mena Suvari, singer Megan Thee Stallion) and are helping to lift the stigma of depression by speaking openly of their experiences—dark periods that are increasingly common across all corners of America.
“I want everyone to know that depression is treatable, and treatment works,” Fetterman said earlier this year. “This isn’t about politics. Right now, there are people who are suffering with depression in red counties and blue counties. If you need help, please get help.”
A lot of people need help. Whether they can find it is another question.
Millions of Americans struggle silently with the disorder, damaging their overall health and shaving years off their expected lifespans. Some may be afraid or unwilling to face ridicule given lingering stigma associated with the disorder, others simply can’t find or afford care or don’t know where to turn. Wait times for mental health services have ballooned to six weeks on average, and months in some parts of the country. Insurance plans often don’t cover the visits or are otherwise highly restrictive.
In the end, only about half of people who need treatment for depression actually receive it, I’ve reported previously.
“Depression is the leading mental health challenge in the US,” said professor Eileen Anderson, EdD, director of education, bioethics and medical humanities at Case Western Reserve University’s School of Medicine. “Depression is now the №1 global burden of health, eclipsing problems like heart disease and HIV,” Anderson added. “Almost everyone knows someone they love who has struggled mightily with depression.”
This overview is the first in a series of Wise & Well articles exploring the depth, breadth, nuances and mysteries of America’s depression crisis.
Especially in America
Globally, about 5% of people suffer clinical depression during any given year, according to the World Health Organization. For many years now, the disorder has been recognized as the leading cause of poor health and disability around the world.
But rates in the United States, by all accounts, are notably higher… and growing. According to WHO estimates, Americans are tied for the second most depressed people, though the percentage differences between most nations are relatively small, and the health infrastructures in the United States and other developed nations are better equipped to diagnose depression, leading to higher apparent rates here than in some countries where it may be just as prevalent but diagnosed less often. Still…
“The only country with higher rates of depression than the US is Ukraine,” Anderson pointed out. “Obviously armed conflict engenders depression.”
Other data reveal disturbing trends in America, particularly among teens and young adults.
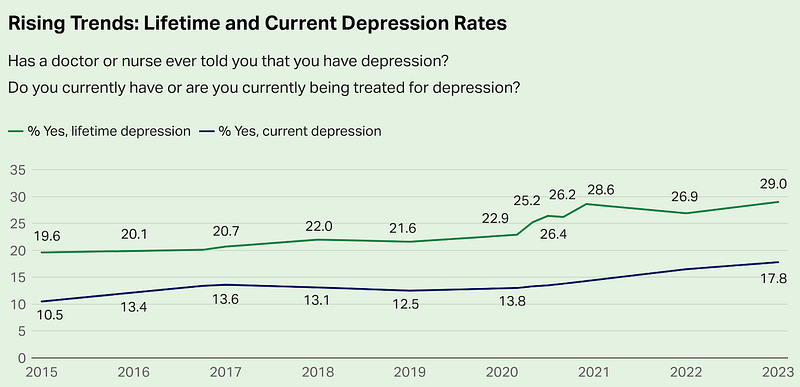
A Gallup poll done earlier this year indicates depression among US adults has been rising since the organization first asked about it in 2015, and rates continue to climb post-pandemic. The results reveal alarmingly high rates of depression at the time the question was asked (17.8% today, up 70% in the past eight years), and even higher rates for lifetime incidence (29% today, up 48% since 2015).
Rates of depression are rising fastest among women, young adults, and Black and Hispanic people, Gallup found.
But are the rates of actual depression increasing? Or are people just becoming more aware of the condition and seeking a diagnosis? Yes, it turns out.
“When it comes to clinically relevant depression, both actual numbers and self-awareness and reporting are increasing,” Anderson told me. “Younger children are being diagnosed with depression, and as lifespan increases, depression is expanding among older adults as well.”
Yet it’s difficult to grasp the true scope of the crisis. Not everyone who struggles with the disorder seeks help and is thereby counted. Nonetheless, the following map and charts — using different data than the Gallup poll — make clear that depression is widespread, leaving no state, county or demographic group untouched.
In the United States, 18.5% of adults say they’ve been diagnosed with depression at some point in their lives, according to a recent analysis by the CDC using data from 2020. The rates vary by county and state, but no county was found to have fewer than one in ten residents who’ve experienced depression.
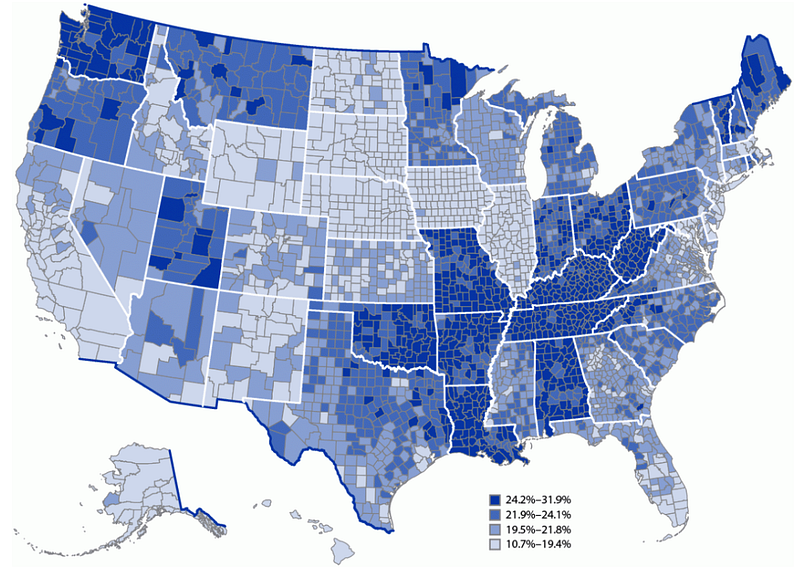
Some of the highest rates were found in the Appalachian region, such as West Virginia, Kentucky and Tennessee, along with Missouri, Oklahoma, and Washington state. Areas with high depression rates tend to also be regions with high rates of chronic diseases like diabetes, arthritis, and heart disease, which can be factors that contribute to depression, according to the CDC. Other contributing factors include low levels of education, lower incomes, high rates of poverty and poor access to healthcare.
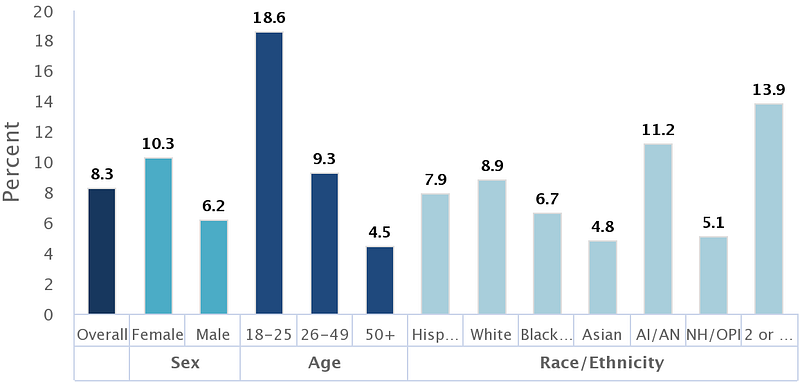
The next two charts, from the National Institutes of Health, offer a snapshot of Americans estimated to have had an episode of major depressive disorder (the diagnosed condition) in the year 2021 — about 8.3% of adults overall, with notably higher rates in women than men, and also among the 18–25 age group:
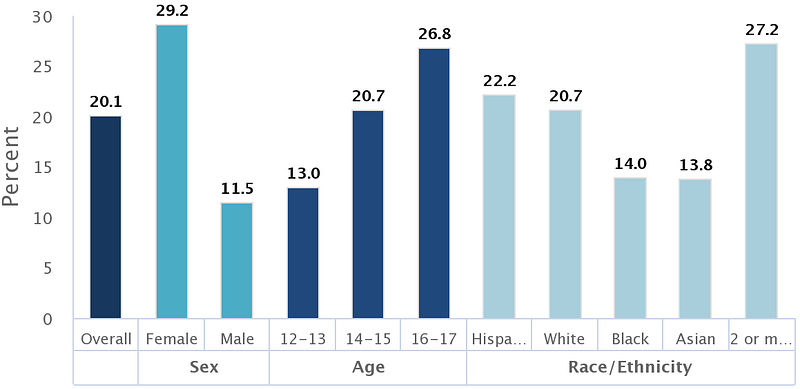
Meanwhile, teen depression has been rising since at least 2005, to the point that rates of depression among youth are higher than in adults — 20.1% overall among adolescents ages 12 to 17, the NIH data finds:
The increase among teens is particularly concerning, because when depression strikes in childhood, it often persists into adulthood.
A more recent analysis only confirms the rising need for care, owing significantly to the pandemic: In-person visits for mental health issues jumped 39% between March 2020 and August 2022, according to a study published last month in the journal JAMA Health Forum. Of those visits, 33% were for depression, and 45% were for anxiety. In the same period, telehealth visits for mental health skyrocketed 10-fold. But this analysis used data on US residents who have insurance through their employers. It doesn’t reveal the unmet needs of others — typically minority groups and lower-income people — who have subpar insurance or none at all.
There’s a “tsunami of unmet need,” says Charles Reynolds, MD, a professor of health sciences at the University of Pittsburgh who co-authored a report on the crisis last year in the journal Lancet that begged for collective action. “We know that most individuals with depression at all stages of life will recover if they obtain adequate support and treatment,” Reynolds said.
What’s going on? Why is the nation so depressed?
The definition of depression is at once precise yet complicated. Grossly oversimplified here, it involves a person experiencing at least five of nine symptoms—including sadness, loss of pleasure in activities, insomnia, feeling worthless, and having suicidal thoughts. Those feelings must be pervasive daily for at least two weeks and impair a person’s ability to function, along with other criteria.
Even among psychiatrists and other mental health experts, the definition and diagnostic criteria for depression are seen as ranging from imperfect to inadequate, while the many potential causes vary tremendously by individual.
Depression can be fueled by a wide range of factors, including but not limited to genetics, biochemistry, anxiety, stress from social isolation, poor health, core personality differences, and economic or cultural challenges. People who face discrimination—whether based on race, ethnicity or gender identity—are far more likely to suffer depression symptoms, multiple studies have found. Likewise, adolescents facing structural racism in their neighborhoods are at higher risk of depression, scientists reported last month.
“I believe now that depression can never be fully grasped by mental health professionals who have not experienced it.” — Richard O’Connor, PhD, author of Undoing Depression
Often, however, there’s a precipitating event — some physical or emotional trauma — that acts as a catalyst for the onset of clinical depression. For many, the pandemic was a catalyst, either directly or through the loss of a job or a loved one or reduced social connections. But many other events can provide ample impetus.
John Fetterman’s plunge into depression was spurred by his stroke, which among other effects damaged his hearing and also auditory pathways that affect his ability to verbally express thoughts that his mind fully grasps. But Fetterman was always a somewhat sad, melancholy guy, his wife told the writer Molly Ball for an article last month in Time Magazine. Some darkness was always there, Ball writes.
Richard O’Connor’s lifelong battle with depression has notably different origins.
At age 15, O’Connor found his mother just after she committed suicide. He suffered powerful episodes of depression in his 20s and again in his 40s. He also got a PhD in social work, became a psychotherapist, and has written several books on mental health.
“I believe now that depression can never be fully grasped by mental health professionals who have not experienced it,” O’Connor writes. “Though I can’t claim to know everything about depression, I have a unique and powerful perspective: as a suicide survivor, as a sufferer myself, as a patient, and as a therapist.”
O’Connor says our behavioral choices, emotional reactions, and daily habits all contribute to setting the stage for a fall into depression. In fact, there are so many elements behind any given individual’s depression that there’s never a single factor that can be called “the cause.”
Depression is a “disease that causes itself,” O’Connor contends in his book Undoing Depression.
“It is a result of current stress acting on a vulnerable individual,” he explains, causing a slide over an invisible cliff, a threshold beyond which a person cannot pull themselves out of the gloom without help. Numerous internal and external elements then feed a vicious circle: self-destructive behavior, stigma, guilt, shame, and chemical changes in the brain, among other challenges. And people unwittingly get good at depression, O’Connor writes, hiding it from the people around them and surviving, even sometimes appearing to thrive, without addressing the root causes of their condition.
Why does all this happen to one person and not another? Why are some people more resilient, others more vulnerable?
“We simply don’t know,” O’Connor writes. But he argues that many of the elements that factor into a person’s depression can be identified and changed — that a depressed person and those around them can have a tremendous effect on the path to recovery by altering mindsets and behaviors, and a person prone to depression can do many things — beyond just medication — to stay away from that invisible cliff in the first place.
Across the population, however, it’s known that income inequality and political conflict contribute to the high rate of American depression, said Anderson, the Case Western Reserve professor, adding: “Those who experience poverty plus discrimination based on gender, race, sexuality or other factors face the highest rates of depression, though no one is immune.”
Risks to health and life itself
Depression comes in many shades of gray. A diagnosis can be termed major depression, bipolar disorder or postpartum depression, among other clinical labels. Avoiding depression isn’t just a matter of being happier or more productive. Far from it. It’s a stark matter of life, health and death.
True depression is far more than a melancholy mood or occasional sadness. We all have blue days now and then, experiencing some of the symptoms of depression. That’s normal. Clinically diagnosable depression can be wholly debilitating.
People with major depression are said to be 30% less healthy overall compared with others, and on average die 10 years sooner. — Blue Cross-Blue Shield
Deanna Barch, PhD, a professor of psychological and brain sciences at Washington University in St. Louis, explained it to me this way:
“A little gloom can help us appreciate good times,” she said. But severe depression, which can come and go in phases or settle in for the long haul, is an entirely different beast. “When people are chronically depressed, they have low motivation, don’t enjoy things, have disrupted sleep, can’t function, can’t concentrate, can’t engage with people.”
Depression can have severe physical side effects, too. Adults ages 18 to 49 who feel depressed are more likely to have a heart attack or stroke, a study earlier this year found.
“When you’re stressed, anxious or depressed, you may feel overwhelmed, and your heart rate and blood pressure rises,” said Garima Sharma, MD, an associate professor of medicine at Johns Hopkins Medicine and senior author of the study. “It’s also common that feeling down could lead to making poor lifestyle choices like smoking, drinking alcohol, sleeping less and not being physically active — all adverse conditions that negatively impact your heart.” The reverse is also true, Sharma and colleagues said: People with heart disease are more likely to feel depressed.
People with major depression are said to be 30% less healthy overall compared with others, and on average die 10 years sooner, a report by Blue Cross-Blue Shield determined.
If there’s one area that’s improved in all this — ironically thanks in part to the pandemic — it’s the reduction in stigma. So even while the incidence of depression is rising, more people are seeking the help they need.
“Stigma against depression was already decreasing before the pandemic, especially in younger generations,” Anderson said. “However, the pandemic — and people’s immense struggling with social isolation along with illness and loss — further removed stigma and increased access to resources. We see interventions and supports expanding at schools, in the workplace, and online.”
Many remedies, no silver bullet
The even better news is that for most people, depression can be prevented or managed — if the right combination of treatments and behavioral changes are recommended based on a full understanding of the elements behind an individual’s condition.
“Depression is among the most treatable of mental disorders,” states the American Psychiatric Association. “Between 80% and 90% of people with depression eventually respond well to treatment. Almost all patients gain some relief from their symptoms.”
Fetterman offers a helpful example of how important an accurate diagnosis is for crafting the right treatment plan.
The psychiatrist overseeing Fetterman’s treatment described the senator not as just sad but flat, unresponsive, lacking any passion or drive, Molly Ball reported in Time. Fetterman had stopped even doing basic personal hygiene. Something had to be fueling his apathy. Eventually, the doctors realized the stroke had caused hearing problems. Meanwhile, he’d lost so much weight, the dose for his heart meds was too high. Hearing aids, medication adjustments and some self-education on depression by Fetterman himself — he read a book about it, helping him regain some self-control over his situation — combined to put him on a path to recovery.
Fetterman’s saga illustrates how the best strategy for any given individual can involve a range of therapies, lifestyle changes, fixes for underlying conditions, and medication when necessary. Every person with depression, or at risk for it, needs individualized help and tailored solutions.
O’Connor emphasizes that point, arguing that medication and conventional psychotherapy don’t go far enough to help most people recover from depression. In Undoing Depression, he lays out a dozen additional steps a person should take via their own initiative, including: learn how to feel your feelings rather than fear them; know that there’s always a reason for mood changes; rise above pessimistic thinking; communicate directly with loved ones about what you’re feeling and what you want.
Meanwhile, there is broad-based agreement on several behavioral changes useful for preventing and battling depression, sometimes in isolation and often in conjunction with each other:
- Improved diet
- More physical activity
- Increase social contact
- Professional therapy
- Better sleep
- Meditation
Last but not least: Antidepressant medication. Prescription meds can be imperative for many people with severe depression, but they tend to be less effective on mild depression, and they don’t work for everyone.
Many experts now say antidepressants are too often the go-to, first and only remedy prescribed for depression, when evidence strongly indicates that physical activity and other tactics can be vital treatment options, in some cases by themselves or often as a complement to medication or other approaches. But in severe cases, telling a patient to hit the gym and sleep better may never succeed without the jumpstart of medication.
Collective action needed
The key message from all mental health experts: People afflicted with depression can’t climb out of it on their own.
Reynolds and his colleagues, in the Lancet report last year, called depression a leading cause of avoidable suffering.
“With sound science, political will, and shared responsibility, depression can be prevented and treated and potentially disabling consequences avoided,” he said. “We must empower people with experience of depression together with families, practitioners, policymakers and civil society to address the tsunami of unmet need — through sharing their experiences to reduce stigma, supporting others with information about the condition and possibilities for help, and advocating for greater resources for evidence-based approaches.”
Finally, it’s crucial to recognize that depression is rarely a one-and-done condition, which makes the rise in US cases so troubling, especially among teens and young adults. People who experience a period of clinical depression at any age, and eventually emerge from it, are at high risk for sliding back in without an ongoing strategy for prevention that involves not just professional help but lifestyle changes. Depression is a condition that can be managed effectively in most cases, and perhaps even cured — at least in a qualified sense.
As O’Connor puts it: “Like alcoholism, depression is a lifelong condition that can be cured only by a deliberate effort to change our selves.”
This article is part of a Wise & Well Special Report: The United States of Depression. If you or a loved one is depressed, it’s vital to talk about it. Because depression increases the risk of suicide, consider calling the confidential National Suicide Prevention Lifeline at 1–800–273-TALK (8255) for English, 1–888–628–9454 for Spanish, or call or text 988. Global support in 44 languages is available from Befrienders Worldwide.




