
Cognitive Therapy for Depression
“I believe that words are strong, that they can overwhelm what we fear when fear seems more awful than life is good.” — Andrew Solomon, The Noonday Demon: An Atlas of Depression

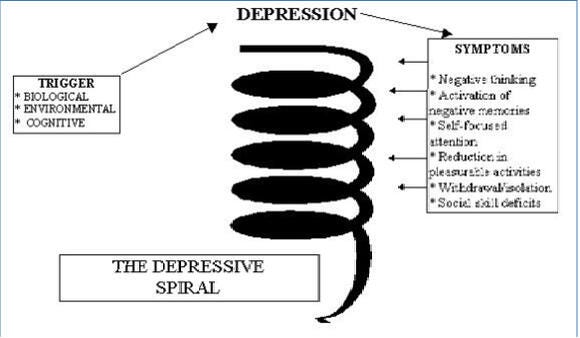
Cognitive therapy for depression is an active, structured, problem-focused, and time-limited approach to treatment which is based on the premise that depression is maintained by negatively biased information processing and dysfunctional beliefs in which both the dysfunctional thinking patterns and the subsequent symptoms serve to exacerbate the depressed mood and perpetuate a mood spiral that increases in both intensity and frequency. (See Figure 1) Treatment is designed to help patients learn to think more adaptively and thereby experience improvements in affect, motivation, and behavior. The efficacy of cognitive therapy for depression has been demonstrated in over 30 clinical trials (Dobson, 1989).
Figure 1 — The Spiral of Depression
Adapted by Robert Westermeyer from: Beck, J. S. (1995). Cognitive therapy: The basics and beyond. New York, NY: The Guilford Press.
The general approach in cognitive therapy for depression involves guiding patients through a number of structured learning experiences. Patients are taught to monitor and write down their negative thoughts and mental images to recognize the association between their thoughts, feelings, physiology, and behavior. They learn to evaluate the validity and utility of these cognitions, test them out empirically, and change dysfunctional cognitions to reflect a more adaptive viewpoint (Sheikhiani & Fakouri, 2012).
As therapy progresses, patients learn to identify, evaluate, and modify underlying assumptions and dysfunctional beliefs that may have predisposed them to depressive reactions. Additionally, the therapist teaches or reactivates adaptive coping skills such as breaking down large problems into smaller, more manageable steps, and decision-making by cost-benefit analysis. Activity scheduling, self-monitoring of mastery and pleasure, and graded task assignments are commonly used early in therapy to help patients overcome inertia and expose themselves to potentially rewarding experiences (Sheikhiani & Fakouri, 2012).
Typical sessions in the cognitive therapy for depression follow a structure that includes a brief check on mood and symptoms, agenda setting, bridging from the previous session, reviewing homework and self-help assignments, discussing issues on agenda, setting new homework, and summarizing and getting feedback from the patient about the session. Cognitive therapists use a variety of strategies and techniques to help depressed patients address their thinking including psychoeducation, guided discovery, Socratic questioning, role playing, imagery, and behavioral experiments.
Patients generally require about eight sessions to gain a reasonable level of mastery with the model and the skills involved. A significant reduction in symptoms often occurs during this initial stage of therapy. The remaining sessions are used to evaluate and modify dysfunctional beliefs that impair functioning and make the patient vulnerable to future depressive episodes, build relapse prevention skills, and discuss termination issues. Many patients show a remission of symptoms in 8–12 sessions. A full course of treatment is considered to be 14–16 sessions although severe cases can take longer. Maintenance of treatment gains is enhanced by occasional booster sessions during the first year after termination.
References
Beck, J. S. (1995). Cognitive therapy: The basics and beyond. New York, NY: The Guilford Press.
Dobson, K.S. (1989). A meta-analysis of the efficacy of cognitive therapy for depression. Journal of Consulting and Clinical Psychology, 57, 3, 414–419.
Sheikhiani, M. & Fakouri, Z. (2012). Management of stress among trainee-teachers through Cognitive-Behavioral Therapy. Journal of Psychological Science, 3 (1), 143–152.