
Caution Needed with Moderna mRNA Vaccine, Especially in Young Males
What the latest large-scale surveillance study says
In biology, it’s always about the dose, even at the nanoscale level. Too much of anything is hardly ever a good thing, and too little of anything is hardly ever helpful.
That’s why pinpointing the threshold — the tipping point —where an effect is effectuated is vital yet tricky because the threshold could differ slightly from person to person. No human bodies work identically, only very similarly. And that slight deviation may be enough to trigger a rare adverse event, such as myocarditis from a dose of the Covid-19 mRNA vaccine.
To state this article’s conclusion early, the risk of myocarditis from Moderna’s mRNA vaccine in young males is small-to-moderate, which is still unlikely to outweigh the numerous risks of Covid-19. (I’d like to say it doesn’t outweigh, not just unlikely, but Omicron seems to cause less severe Covid-19, and the current vaccines are still based on the extinct Wuhan 2019 strain.) But if given a choice, Pfizer’s mRNA or other Covid-19 vaccines is the better choice for young males.
mRNA vaccine dose
Currently, two mRNA vaccines against Covid-19 are available, which are from Pfizer-BioNTech (BNT162b2) and Moderna (mRNA-1273).
The dose of Pfizer’s mRNA vaccine is 0.3 mL (30 micrograms) for those over 12 years old, whereas Moderna’s is 0.5mL (100 micrograms, not 50) for those over 18. (Moderna mRNA vaccine is only authorized for 18 and above.) So, the dose of Moderna’s mRNA vaccine is >3-times the dose of Pfizer’s.
At least two doses of each mRNA vaccine are required, given weeks or months apart, to elicit sufficient immunity. Both were equally efficacious at preventing symptomatic Covid-19 (>90% efficacy) in their clinical trials. But with the emergence of more immune-evasive variants of SARS-CoV-2, such as Delta and Omicron, a third booster shot is needed to retain immunity.
As the dose of Moderna’s mRNA vaccine is higher, its protection against severe Covid-19 from Delta is slightly better than Pfizer’s. Moderna’s mRNA vaccine also remains effective for longer than Pfizer’s over four months. The same pattern likely holds for Omicron, which has overtaken Delta (the dominant variant worldwide before Omicron) in many countries.
Does that mean Moderna’s mRNA vaccine is superior to Pfizer’s? Not quite. The 3x higher dose of Moderna’s mRNA vaccine also comes with a higher risk of myocarditis (inflamed heart muscles) in young people, especially males.
The price
I’ve previously reviewed several surveillance studies on mRNA and DNA vaccine safety from various countries and find that studies from the U.K. are generally the most well-done. The U.K. has one of the best healthcare systems globally, so their surveillance system could probably catch rare events with higher precision than most other countries.
Now, researchers from the U.K. have published another vaccine surveillance study — the largest one about cardiac adverse events to date — in Nature Medicine last month. Herein, Dr. Patone et al. collected data from everyone above the age of 16 who were vaccinated (38.5 million people) or tested positive for Covid-19 by PCR (3 million people) in the U.K. Among those vaccinated, about 20 million got AstraZeneca’s DNA vaccine, 16 million got Pfizer’s mRNA vaccine, and 1 million got Moderna’s mRNA vaccine.
A self-control design was used, where individuals act as their own controls; for example, the unvaccinated and vaccinated groups are derived from the same person at pre- and post-vaccination periods. This design naturally controls for the countless number of variables that differ between individuals, such as health behavior or status, genetics, or occupation.
They examined three cardiac adverse events: myocarditis (inflamed heart muscles), pericarditis (inflamed heart linings), and arrhythmia (abnormal heart rate or rhythm). And results revealed an increased risk of:
- myocarditis within 28 days of the (i) first dose of AstraZeneca’s DNA vaccine (1.3-times), (ii) first dose of Pfizer’s mRNA vaccine (1.3-times), (iii) first and second doses of Moderna’s mRNA vaccine (3- and 9.8-times, respectively), and (iv) SARS-CoV-2 infection (9.8-times).
- arrhythmia within 28 days of the (i) second dose of Moderna’s mRNA vaccine (1.5-times) and (ii) SARS-CoV-2 infection (5.4-times).
- pericarditis within 28 days of SARS-CoV-2 infection (2.8-times).
Focusing on myocarditis only, their result tables can be hard to understand, so I have adapted their hard-to-read data into a single table here:
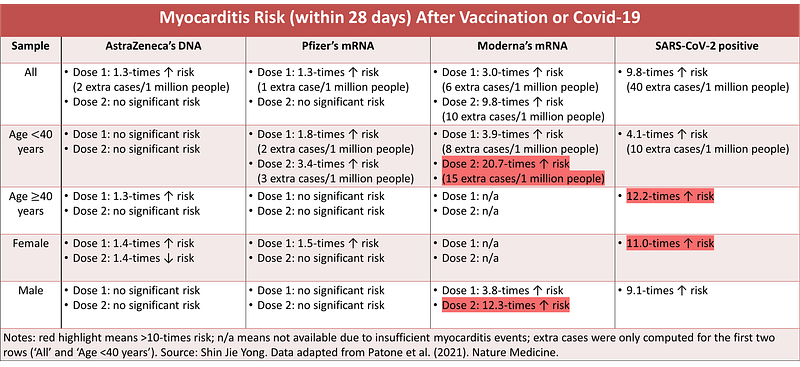
So, myocarditis risk is greatest from the second dose of Moderna's mRNA vaccine, at 20.7-times in 16–39-year-olds and 12.3-times in males. It’s thus apparent that for younger males, the risk of myocarditis from Moderna’s mRNA vaccine is greater than SARS-CoV-2 infection.
Yes, for younger males only. Females and those ≥40 years still face a much greater risk of myocarditis (and other cardiac disorders) from SARS-CoV-2 than vaccines. Neither Pfizer’s nor Moderna’s mRNA vaccines increased the risk of myocarditis in individuals ≥40 years.
(Dr. Patone et al. also computed the risks of anaphylaxis (a vaccine-specific allergic reaction) and celiac disease (a gluten-specific autoimmune disease) to serve as positive and negative controls, respectively. As expected, anaphylaxis risk increased on the first day of vaccination, whereas no overall risk change was found with celiac disease, thus validating their analyses and results.)
Other surveillance studies have also reported elevated myocarditis risk from mRNA vaccines, mainly from the second dose in younger males:
- Ministry of Health, Israel: Within 30 days of the second dose of Pfizer’s mRNA vaccine (n = 5M), a 2.4-times increased risk of myocarditis was noted (1.6 excess cases per 100K people). This risk is highest in males between 16–19 (9-times, 13.7 excess cases per 100K people) and 20–24 (6.1-times, 9.6 excess cases per 100K people) years.
- Vaccine Safety Datalink, the U.S.: Within 21 days of either Pfizer’s or Moderna’s mRNA vaccine (n = 6.2 million), a 9.8-times increased risk of myocarditis (6.3 excess cases per 1M doses) was noted in those aged 12–39 years only. This risk is greatest within seven days of the second dose (10.4-times; 11.2 excess cases per 1M doses).
- Danish Vaccination Register, Denmark: Within 28 days of Pfizer’s mRNA vaccine (n = 3.5M), no risk of myocarditis was found. But within 28 days of Moderna’s mRNA vaccine (n = 0.5M), a 6.1-times elevated risk of myocarditis was noted (4.2 excess cases per 100K people), which further increased in males and (6.3 excess cases per 100K people) and 12–39 year-olds (5.7 and 6.3 excess cases per 100K people).
The most probable explanation for the greater risk of myocarditis from Moderna’s mRNA vaccine than from Pfizer’s is the dose. As mentioned at the start, the dose of Moderna’s mRNA vaccine is thrice that of Pfizer’s. As follows, Moderna’s mRNA vaccine is known to elicit more potent antibody immune responses than Pfizer’s. And myocarditis is also immune-mediated.
A mice study showed that intravenous (into the vein) injection of mRNA vaccine caused myocarditis (and spike protein expression on heart muscle cells), but not intramuscular (into the muscles) injection. So, traces of mRNA vaccine entering the veins by accident during intramuscular injection might induce spike protein expression on heart muscles, triggering myocarditis. The faster metabolism of young males and the pro-inflammatory effects of testosterone probably aid this process.
I’ve written about this in more detail here: “Heart Inflammation From mRNA Vaccine: Probable Causes and Precautions.”
The broader implications
Thankfully, myocarditis is rare. An increase of x (e.g., myocarditis) relative to a rare event will still be rare. This is reflected by the absolute increase of only 15 extra myocarditis cases per 1 million people who got Moderna’s mRNA vaccine — despite a relative increase in risk by over 20-times — in those less than 40 years old in the U.K. study (Patone et al.).
Whether this risk is small or moderate is up to the interpreter, but it’s by no means a huge one. The remaining 999,985 vaccinated people got no myocarditis after all.
But risk means nothing if it actually happens to a person. So, any risk exposure — even though it’s by vaccination — is best avoided. To a young male, therefore, Moderna’s mRNA vaccine may not be the best one to take, especially at the second dose and perhaps at the third dose too.
Speaking of the third dose, the findings discussed above also question the safety of repeated mRNA vaccinations (boosters) against Covid-19. No studies have computed the risk of myocarditis from the third or fourth mRNA vaccine dose. But the risk of myocarditis is likely to increase with each consecutive dose, given that the second dose comes with a higher myocarditis risk than the first dose and that immune responses strengthen with each dose.
Previously in an article in The Lancet in September 2021, researchers from the FDA, WHO, and other institutions have already cautioned against the use of Covid-19 vaccine boosters, writing that:
Although the benefits of primary COVID-19 vaccination clearly outweigh the risks, there could be risks if boosters are widely introduced too soon, or too frequently, especially with vaccines that can have immune-mediated side-effects (such as myocarditis, which is more common after the second dose of some mRNA vaccines…). If unnecessary boosting causes significant adverse reactions, there could be implications for vaccine acceptance that go beyond COVID-19 vaccines.
So, Moderna’s mRNA vaccine may be best allocated to the older age groups who are not at risk of mRNA vaccine-related myocarditis. Whereas younger people, particularly males, may be better off taking Pfizer’s mRNA or other Covid-19 vaccines, if possible.
Even if it’s not possible, Moderna’s mRNA vaccine is still likely to bring more benefits than harm, given that the risks of Covid-19 are manifold, not just myocarditis. Covid-19 is known to increase the risk of long-term issues, such as long-Covid (fatigue, brain fog, breathlessness, etc.) and other chronic diseases (e.g., heart attack, stroke, lung fibrosis, diabetes, etc.). Plus, most cases of mRNA vaccine-related myocarditis is readily recoverable:
- In the U.K. study, the median and average hospitalization period for post-vaccine myocarditis was 3–4 days and 5–8 days, respectively. So, mRNA vaccine-related myocarditis is a short-term disease.
- In the Denmark study, in those who developed mRNA vaccine-related myocarditis, 40-58% were hospitalized, 2% developed heart failure, and 0% died. But in unvaccinated people who got myocarditis (control group), 48% were hospitalized, 4.5% developed heart failure, and 2% died.
- In another Israel study with 2.5 million people vaccinated with Pfizer’s mRNA vaccine, 54 developed myocarditis, of which 76% were mild, 22% were moderate, and 2% (only one person) were severe with cardiogenic shock. About 80 days after myocarditis, only 2% were readmitted to the hospital, and 2% died of an unknown cause. The rest were fine.
Still, mRNA vaccine-related myocarditis is not a disease with a 0% mortality rate. Its long-term consequences — albeit unlikely to pose any based on the Israel study with 80 days of follow-up — are also unclear.
Another concern is that the U.K. study only investigated three cardiac events — myocarditis, pericarditis, and arrhythmia — from Moderna’s mRNA vaccine. But there are also signals of slightly increased risks of stroke and blood clots from Pfizer’s mRNA vaccine in two other U.K. surveillance studies, conducted by the same research team of Patone et al. If Moderna’s mRNA vaccine delivers a greater risk of myocarditis than Pfizer’s, the same situation might apply to stroke and blood clots, but this is pure speculation for now.
But other surveillance studies from Israel, the U.S., France, and Scotland found no association between mRNA vaccine and stroke and blood clots. Among these, only the U.S. study examined both Pfizer’s and Moderna’s mRNA vaccines as one group; the rest only examined Pfizer’s mRNA vaccine. I’ve also previously discussed these surveillance studies here: “Can We Trust the Covid-19 Vaccines? What Phase IV Surveillance Studies Show.”
So, it’s apparent that large-scale surveillance studies on Moderna’s mRNA vaccine safety are lacking, which is why we may need to approach the use of Moderna’s mRNA vaccine more carefully, especially in young males.
If you have made it this far, thank you. Subscribe to my Medium email list here. If you want to become a member to get unlimited access to Medium, you can use my referral link, and I will receive a small commission at no extra cost to you. You can also tip me below if you are feeling generous today, and I’ll appreciate it. Paying bills with science writing isn’t easy, so I’ll appreciate any help I can get.





