
Can We Trust the Covid-19 Vaccines? What Phase IV Surveillance Studies Show
Scientific studies support vaccine safety, but certain individual reports don’t. Which side to trust?
A randomized controlled trial (RCT) is the gold-standard method for testing the safety and efficacy of a drug or biologic in humans. Because of RCTs, we know that the Covid-19 vaccines are safe and effective compared to the control group.
Beyond the clinical trial’s control group in the general population, however, we rely on observational studies to monitor vaccine safety and efficacy. We call this post-licensure or post-marketing surveillance. But as observational study design is inferior to RCT, can we trust that the Covid-19 vaccines are safe and effective outside of the RCTs?
As covering both vaccine safety and effectiveness are too extensive, I’ll focus on safety, especially the most commonly used mRNA and DNA vaccines.
Individual voices have raised concerns about vaccine safety. I’ll not name names here, but you most probably have heard or seen articles or videos declaring that Covid-19 vaccines are dangerous. They commonly cite the Vaccine Adverse Event Reporting System (VAERS), a surveillance system in the U.S. that relies on voluntary reporting from healthcare providers or patients. It’s basically a collection of anecdotes, which have been useful in catching vaccine-related adverse events early.
So, can we still trust that the Covid-19 vaccines are safe outside of the RCTs?Yes, because several large surveillance studies conducted in the real world have shown that risks associated with vaccines are minimal, which are far lower than the risks of Covid-19.
Why Phase III Clinical Trials Aren’t Enough
If a drug candidate works safely in cell culture and animal studies, the pharmaceutical company may apply for permission from the Food and Drug Administration (FDA) to begin clinical trial testing on humans, starting from phase I to IV.
Phase I clinical trial tests the drug at various doses in a small group of people to ensure and determine a safe dose. Phase II then tests if the drug works via a randomized controlled trial (RCT), usually in over a hundred participants. Next, phase III tests the drug in a larger group of people, usually thousands. Drug safety is also monitored in phases II and III.
The FDA will review all the clinical trial data again before approving or authorizing the drug for public use. Phase IV then observes how the drug works in the real world, outside of the clinical trials.
Phase IV is necessary because the drug may behave differently in the real world than in controlled conditions. RCTs have strict inclusion and exclusion criteria to ensure that results are more likely to be reproducible and to minimize potential harm in vulnerable populations.
The phase III trial of Pfizer’s mRNA vaccine, for example, stated:
“Adults 16 years of age or older who were healthy or had stable chronic medical conditions…were eligible for participation in the trial. Key exclusion criteria included a medical history of Covid-19, treatment with immunosuppressive therapy, or diagnosis with an immunocompromising condition.”
Phase IV is also needed because RCTs don’t study the entire population. The sample size will always be insufficient, especially if the drug is intended for general use, such as Covid-19 vaccines.
The phase III trial of Pfizer’s mRNA vaccine injected 21,720 participants with the mRNA vaccine and 21,728 with placebo and found that the vaccine posed no additional harm compared to the placebo. But this is true within that 21,728 participants only who were healthy or had stable diseases.
Plus, a sample size of 20,000 is only enough to detect an adverse event that occurs at the rate of 1–3 cases in 2000 people. (Detect as in showing statistically significant results at P < 0.05.) To detect an adverse event with an incidence rate of 1 in 10,000, at least 30,000 participants are needed.
The sample size limit explains why the phase III trials of Covid-19 vaccines have missed all the rare adverse events that were later detected by phase IV surveillance systems — such as mRNA vaccine-related myocarditis, DNA vaccine-related thrombotic thrombocytopenia, and DNA vaccine-related Guillain-Barre syndrome.
(The phase III trials of Moderna’s mRNA and Novavax’s subunit vaccines also have similar inclusion and exclusion criteria as Pfizer’s mRNA vaccine. The phase III trial of AstraZeneca’s DNA vaccine only included healthy adults aged 18–55 years. Participants in the phase III trial of Johnson & Johnson’s DNA vaccine were also mostly healthy 18–59-year-old adults who did not have medical conditions associated with increased risk of severe Covid-19. These phase III trials have about 15,000 to 30,000 participants.)
What phase IV surveillance studies show
To this end, I search PubMed, a biomedical literature database, with the keywords “(nation* OR surveillance OR cohort) AND (safe* OR risk) AND (BNT162b2 OR ChAdOx1nCoV-19 OR mRNA-1273 OR Ad26.COV2.S).
After going through them, there are six notable large cohort studies on mRNA vaccine safety — three of them also examined DNA vaccine —that serve as phase IV surveillance studies. I picked those six because they have proper control (or comparison) groups, which most other studies don’t.
*If you are only interested in seeing the top three surveillance studies, skip to the table below, where the death % is also presented.
1. Clalit Health Services (CHS) database of Israel (Barda et al. ); investigated 25 different adverse events:
- Within 21 days of the first/second dose (total 42 days; n = 884,828), Pfizer’s mRNA vaccine was associated with increased risks of myocarditis (3.2-times; 2.7 excess events per 100,000 people), appendicitis (1.4-times; 5 excess), lymphadenopathy (2.4-times; 78.4 excess), and herpes zoster infection (1.4-times; 15.8 excess), but decreased risks of anemia (1.2-times; 18.7 fewer events per 100,000 people), acute kidney injury (1.6-times; 4.6 fewer), intracranial hemorrhage (1.5-times; 2.9 fewer), and lymphopenia (1.7-times; 0.9 fewer). And it’s unrelated to 17 other adverse events (stroke, blood clots, etc.) investigated.
- Within 42 days of a positive test (n = 172,106), SARS-CoV-2 was associated with increased risks of myocarditis (18.3-times; 11 excess events per 100,000 people), acute kidney injury (14.8-times; 125 excess), pulmonary embolism (12.1-times; 61.7 excess), intracranial hemorrhage (6.9-times; 7.6 excess), pericarditis (5.4-times; 10.9 excess), myocardial infarction (4.5-times; 25.1 excess), deep-vein thrombosis (3.8-times; 43 excess), and arrhythmia (3.8-times; 166 excess). But it’s unrelated to 17 other adverse events investigated.
- Key limitations: (i) Certain populations, such as health care workers and residents of long-term care facilities, were excluded. (ii) Some out-of-network hospital diagnoses might have been missed.
2. Vaccine Safety Datalink (VSD) database of the U.S. (Klein et al.); investigated 23 different adverse events:
- Within 21 days of receiving a dose of either Pfizer’s or Moderna’s mRNA vaccine (n = 6.2 million people), the vaccine was associated with anaphylaxis (5 cases per 1 million doses; risk n/a as anaphylaxis is a vaccine-specific condition) and myocarditis/pericarditis (9.8-times increased risk; 6.3 excess cases per 1 million doses; in younger subgroup only). And it’s unrelated to other adverse events (e.g., Guillain-Barre syndrome, stroke, blood clots, etc.) examined.
- Key limitations: (i) The 95% confidence intervals of six adverse events were wide, indicating limited statistical power and sample size for certain rare events. A wide confidence interval means we are unsure where the true average lies (e.g., 95% confident that it’s 10–15% (narrow) vs. 10–150% (wide)). (ii) Only adverse events were medically attended were included, so the risks of some events might be underestimated if health care was not sought.
3. VSD database of the U.S. (Xu et al.); investigated deaths unrelated to Covid-19:
- In deaths occurring within 30 days of Covid-19 absence, Pfizer’s (n = 4.6 million) mRNA, Moderna’s (n = 2.6 million) mRNA, and Johnson & Johnson’s DNA (n = 0.34 million) vaccines were associated with a reduced risk of non-Covid-19-related deaths (1.5- to 1.7-times).
- Key limitations: (i) It’s an observational study prone to confounding, such as healthier behaviors in the vaccinated group. (ii) Cause of death was not examined. (iii) VSD only has data of about 3% of the U.S. population, so results may not be readily generalizable.
4. National Immunisation Management System (NIMS) database of the U.K. (Hippisley-Cox et al.); investigated seven cardiovascular disorders:
- Within 28 days of the first dose (n = 9.5 million), Pfizer’s mRNA vaccine was associated with increased risks of ischaemic stroke (1.1-times; 143 excess events per 10 million people), arterial thromboembolism (1.1-times; excess n/a), cerebral venous sinus thrombosis (3.6-times; excess n/a). And it’s unrelated to the other cardiovascular disorders examined.
- Within 28 days of the first dose (n = 19.6 million), AstraZeneca’s DNA vaccine was associated with increased risks of thrombocytopenia (1.3-times; 107 excess events per 10 million people), cerebral venous sinus thrombosis (4-times; 7 excess), and venous thromboembolism (1.1-times; 66 excess). And it’s unrelated to the other disorders examined.
- Within 28 days of a positive test (n = 1.8 million), SARS-CoV-2 was associated with increased risks of all cardiovascular disorders examined: thrombocytopenia (1.5- to 14-times; 934 excess events per 10 million people), venous (3.4- to 13.9-times; 12,614 excess) and arterial (1.3- to 6.6-times; 5,573 excess) thromboembolism, cerebral venous sinus thrombosis (13-times; 20 excess), ischaemic stroke (1.3- to 3.9-times; 1,699 excess), myocardial infarction (1.9- to 8-times; 3,633 excess), and other blood clotting disorders (2.7- to 5.6-times; 540 excess).
- Key limitations: (i) Only completed hospital admissions were included, so ongoing hospitalizations by the study’s end date were excluded. (ii) Medical diagnoses were not adjudicated (i.e., the formal process of verifying a diagnosis or claim of a healthcare provider).
5. NIMS Database of the U.K. (Patone et al.); investigated seven neurological disorders:
- Within 28 days of the first dose (n = 12 million), Pfizer’s mRNA vaccine was associated with an increased risk of hemorrhagic stroke (1.4-times; 60 excess cases per 10 million people). But it’s unrelated to six other neurological disorders examined.
- Within 28 days of the first dose (n = 20 million), AstraZeneca’s DNA vaccine was associated with increased risks of Guillain–Barré syndrome (2.9-times; 38 excess cases per 10 million people), Bell’s palsy (1.3-times; excess n/a), and myasthenic disorder (1.6-times; excess n/a). But it’s unrelated to four other disorders examined.
- Within 28 days of a positive test (n = 2 million), SARS-CoV-2 infection was associated with increased risks of all neurological disorders examined: central nervous system demyelination (2.6- to 19.3-times; excess n/a), encephalitis/meningitis/myelitis (2.1- to 38.6-times; 123 excess cases per 10 million people), Guillain-Barre syndrome (3.5- to 33.4-times; 145 excess), Bell’s palsy (2.2-to 33.2-times; excess n/a), myasthenic disorder (2.8- to 61.3-times; 163 excess), hemorrhagic stroke (2- to 12.4-times; excess n/a), and subarachnoid hemorrhage (2.2- to 24.2-times; excess n/a).
- Key limitations: Only neurological disorders leading to hospital admissions or deaths were included, so the risks of some events might be underestimated if health care was not sought.
6. National Health Service (NHS) database of Scotland (Simpson et al.); investigated five blood clotting disorders:
- Within 28 days of the first dose (n = 1.7 million), AstraZeneca’s DNA vaccine was associated with increased risks of immune thrombocytopenia (5.8-times; incidence of 1.3 cases per 100,000 doses), arterial thromboembolism (1.2-times), and hemorrhagic events (1.5-times) compared to unvaccinated control, but the latter two became insignificant in self-control design. And it’s unrelated to venous thromboembolism and non-immune thrombocytopenia.
- Within 28 days of the first dose (n = 0.8 million), Pfizer’s mRNA vaccine was not associated with any blood clotting disorders examined.
- Key limitations: (i) The AstraZeneca’s DNA vaccine group lacks young people as this vaccine is now promoted for older age groups to minimize risks of blood clots in younger age groups. (ii) The case-control (not self-control) design may have unaccounted confounding variables that may overestimate the effect size.
***
[Extra] Other less extensive surveillance studies with control groups:
- Ministry of Health database, Israel (Mevorach et al.): Pfizer’s mRNA vaccine was associated with an increased risk of myocarditis (2.4-times), which was highest in 16–19-year-old males (9-times) (n = 9.3 million; 21 days following either dose).
- Meuhedet Health Maintenance Organization (MHMO), Israel (Shasha et al.): Pfizer’s mRNA vaccine was not associated with Guillain-Barre syndrome, Bell’s palsy, and herpes zoster infection (n = 233,156; 3–5 weeks following either dose).
- TriNetX Analytics Network, the U.S. (Birabaharan et al.): Pfizer’s mRNA vaccine was not associated with herpes zoster infection (n = 1.3 million; 28 days following either dose).
- COVID-19 Vaccine Adverse Event online Reporting System, Hong Kong (Wan et al.). Sinovac’s inactivated vaccine was associated with an increased risk of Bell’s palsy (2.4-times; 4.8 excess cases per 100,000 person-years; n = 451,939), but not Pfizer’s mRNA vaccine (n = 537,2015) (42 days following either dose).
- Surveillance of Adverse Events Following Vaccination in the Community (SAEFVIC), Australia (Gordon et al.): AstraZeneca’s DNA vaccine was associated with an increased risk of immune thrombocytopenia (2-times; n = 2 million), but not Pfizer’s mRNA vaccine (n = 1.6 million) (28 days following either dose).
- French National Health Data System, France (Jabagi et al.): Pfizer’s mRNA vaccine was not associated with myocardial infarction, stroke, and pulmonary embolism in those over 75-years-old (n = 3.9 million; 14 days following either dose).
Are phase IV surveillance studies reliable?
Judging from these surveillance studies, it’s very clear that SARS-CoV-2 infection or Covid-19 is a much larger threat than vaccines. Risks of most adverse events are many times higher in the infected versus vaccinated group (see bullet points #1, #4, and #5).
Among those surveillance studies, the two U.K. studies (Patone et al. and Hippisley-Cox et al.) and the Scotland study (Simpson et al.) have the least limitations in study design. The exclusion and inclusion criteria of the two U.K. studies (published separately here) are unbiased and simple:
“All patients of all ages will be included in the analyses since all patients are eligible to be considered for COVID-19 vaccination or likely to become so over time. Patients will be excluded if they have had three or mode vaccines or a combination of more than one vaccine type.”
Similarly, the Scotland study protocol (published separately here) included everyone registered with a general medical practice, representing 91% of the Scottish population. As the study authors wrote:
“Almost all residents in Scotland are registered with a general practice and have a unique Community Health Index (CHI) number used by NHS Scotland. We used the CHI number to deterministically link all datasets with vaccination records in Public Health Scotland…together, these captured all vaccination records, including those vaccinated in general practices, community vaccination hubs and other settings, such as care homes and hospitals in Scotland.”
***
Whereas the Israel study using the CHS database omitted several groups of people — such as residents of long-term care facilities, people confined to their homes for medical reasons, and health care workers— because of the inability to control for confounding variables in these people.
The Israel study follows a matching design, where a group of vaccinated people was carefully matched to unvaccinated people in terms of age, sex, residence, socioeconomic status, population sector, comorbidities, and pregnancy status. As healthcare workers and long-term care facility residents are at high risk for severe Covid-19 and prioritized for vaccination, there were not enough of them left in the unvaccinated group.
In contrast, the U.S. (Klein et al.) and U.K. (Patone et al. and Hippisley-Cox et al.) studies use a self-control design, where the vaccinated/unvaccinated and infected/uninfected groups consist of the same people at different time points. Patone et al. and Hippisley-Cox et al. compared risks at post-vaccination vs. pre-vaccination, whereas Klein et al. compared risks at 0–21th vs. 22–42th day of vaccination.
This design helps control for nearly all variables that could have differed from person to person. In other words, the risk of x is compared to oneself — at past self (pre-vaccination) or future self (sometime after vaccination) — rather than to someone else with similar baseline characteristics.
***
But the U.S. studies (Klein et al. and Xu et al.) have another limitation with its database, the Vaccine Safety Datalink (VSD) that collects vaccine-related data from several healthcare organizations at nine sites in the U.S.
VSD actively collects data and doesn’t rely on voluntary reporting (passive surveillance) like VAERS. Both VSD and VAERS are among the main vaccine surveillance systems in the U.S.
Such an active system of VSD is suitable for performing statistical analyses on vaccine safety — such as the prevalence, risks, and outcomes of a vaccine-related adverse event — as the data is collected systematically.
But VSD has one limitation: it tends to miss very rare events. For instance, the early detection of blood clotting concerns from the Johnson & Johnson’s DNA vaccine was detected by VAERS; VSD missed it.
After all, VSD only collects data from nine sites — containing data of about 3% of the U.S. total population only — while anyone can report to VAERS. At the end of November 2021, about 60% of the U.S. population is fully vaccinated (with another 10% that is partially vaccinated). So, VSD’s coverage is minimal, lacking socioeconomic diversity. This limitation probably explains why certain adverse events in the U.S. study had wide confidence intervals (see the 2nd bullet point above).
This is not to say that VSD data is unreliable, however. As VSD prioritizes information quality over quantity, we can be assured that the underlying raw data is trustworthy. It’s just that whether the VSD data (and results) apply to other sites in the U.S. or other countries is debatable.
***
So, the two U.K. studies (Patone et al. and Hippisley-Cox et al.) and the Scotland study (Simpson et al.) provide the most robust evidence on vaccine safety in the general population. They examined how the vaccines work in almost everyone who got the vaccine, a high-quality surveillance research. So, their findings should be the closest to the truth we have.
What were their findings again? Based on the bullet points above, I summarized the three top surveillance studies in a table here, with the added death rate information I extrapolated from the raw data:
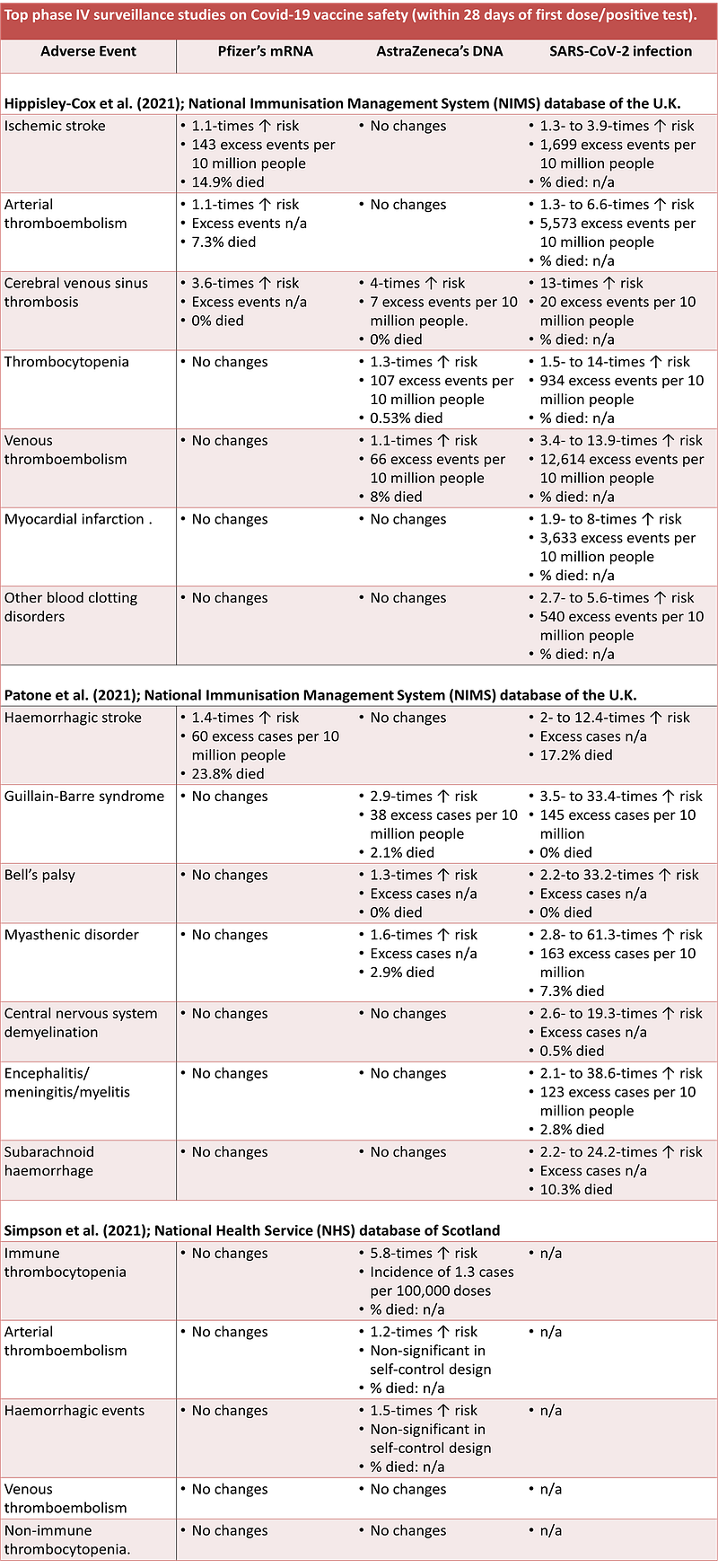
As authorities have acknowledged, AstraZeneca’s DNA vaccine comes with the risk of blood clotting disorders and Guillain-Barre syndrome, especially in younger females. As a result, several European countries have minimized or banned the use of AstraZeneca’s vaccine in younger age groups.
Surprisingly, Pfizer’s mRNA vaccine is also associated with risks of blood clots and stroke — but not the other neurological disorders — in the U.K. NIMS database only. The Scotland NHS database did not find such risks.
After reading the discussion sections of the three surveillance studies, no explanations were written on the link between Pfizer’s mRNA vaccine and stroke and blood clots. Plausible reasons I can think of are:
- Differences in database characteristics and/or statistical analyses between the U.K. NIMS and Scotland NHS studies.
- The link between Pfizer’s mRNA vaccine and stroke is not robust, which may not always be replicable. In fact, three other surveillance studies — such as the Israel CHS (Barda et al., 2021), U.S. VSD (Klein et al., 2021), and French National Health Data System (Jabagi et al., 2021) — reported that Pfizer’s mRNA vaccine was unrelated to stroke and blood clots.
- Some inherent traits— such as genetic or environmental factors — that predispose U.K. residents (and not Scotland’s) to develop stroke and blood clots after getting Pfizer’s mRNA vaccine.
Even the best surveillance studies are not perfect
One limitation is that they can’t prove anything. Surveillance studies are observational in design, which has no randomization. Randomized controlled trials (RCTs), in contrast, randomize people into either the experimental or control group. Such randomization negates the countless variables that differ from person-to-person, ensuring that results are strictly due to the experimental condition. Observational studies control for controllable factors only, such as age and sex; genetic, behavioral, environmental, and cultural factors are almost never accounted for.
The second limitation is that not all adverse events are studied. The three top surveillance studies (Patone et al., Hippisley-Cox et al., and Simpson et al.) did not examine myocarditis (heart inflammation), for example. Myocarditis is a known risk of mRNA vaccines, especially in younger males. So, we can’t be sure that the other uninvestigated adverse events are not linked to the vaccines from these three surveillance studies.
Third, each of the surveillance studies is limited to one geography only. So, we can’t be 100% certain that the same pattern applies to other countries with different socioeconomic settings. For example, the U.K. (including Scotland) has arguably the best healthcare system in the world, so their NIMS and NHS databases might be able to catch adverse events with higher precision. But most other countries lack such an advanced healthcare system, so their analyses may show different results from the U.K.
Even though those surveillance studies are not perfect, their findings are the closest to the truth we have. In physics, it’s a common saying that there are no absolute truths in science, only approximate truths.
What’s the approximate truth about Covid-19 vaccines then? Answer: mRNA and DNA vaccines are safe for the vast majority.
For instance, based on the top three surveillance studies (see the table above), the adverse event that produced the highest excess cases is ischaemic stroke from Pfizer’s mRNA vaccine at 143 excess cases per 10 million people. So, if we vaccinate 10 million people with Pfizer’s mRNA vaccine, we would see 143 more stroke cases (of which 14.9% will die) than usual. But put it another way, the remaining 9,999,857 people did not develop stroke after getting Pfizer’s mRNA vaccine.
I said the vast majority. As humans are complex biological creatures, some outliers are bound to occur in our civilization, who may react to vaccines negatively, or the vaccine might trigger something dangerous in them.
After all, we can’t deny that the vaccines are associated with excess cases of several adverse events, of which some have even died, from the top three surveillance studies described above. This is where frightening anecdotes of people dying or getting severely ill after vaccination might come from.
But it’s equally if not more important to remember that much more people would be badly affected by Covid-19 if it wasn't for the vaccines. Current Covid-19 statistics stand at over 260 million cases and 5 million deaths.
Trust the surveillance studies or VAERS?
Speaking of anecdotes, the Vaccine Adverse Event Reporting System (VAERS) is basically a collection of anecdotes from voluntary reporting of healthcare professionals or patients in the U.S.
*Reminder: All vaccines mentioned in this section refer to Covid-19 vaccines.
VAERS is arguably the backbone of the dangerous vaccine narrative. Several independent people have performed their own analyses and interpretations of VAERS to show how dangerous the vaccines are.
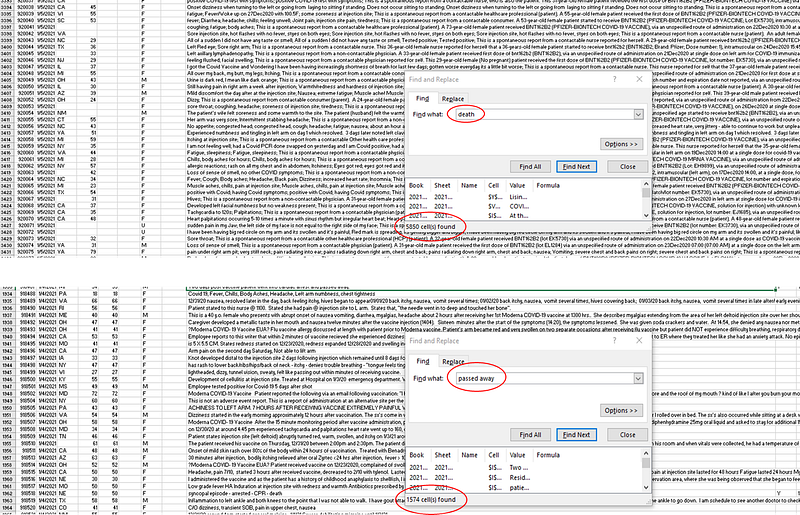
Anyone can access VAERS raw data. I downloaded its 2021 data (as of 5 December 2021) and simply ctrl+F “death” and “passed away” gave me 5,850 and 1,574 hits, respectively. Not all hits are death cases because some hits said the case didn’t result in death. But compiling enough descriptions of the actual death cases produces a scary depiction of the situation (like the image shown in the intro above).
***
I wrote about VAERS back in July 2021: Underreporting and Post-Vaccine Deaths in Vaccine Adverse Event Reporting System (VAERS) Explained. The points I raised back then still stand to this day. So, this section is a summary of my past article, with some newer input from other sources.
First, we have seen a huge spike in vaccine-related adverse events and deaths in VAERS during the past year. Then some people assumed that the vaccine caused these deaths, at least most or a proportion of them.
Sure, things can be more complicated than this. But this observation (the spike in numbers) and assumption (vaccines likely caused them) are arguably the foundation of the dangerous vaccine narrative based on VAERS. If this foundation is unreliable, the downstream complicated stuff becomes unreliable too.
For one, it’s expected that we see a huge spike in VAERS report this past year, given the sheer number of vaccines distributed. Plus, the numerator (number of vaccine-related adverse events or deaths) is misleading without the denominator (number of vaccine doses given). Second, VAERS does not contain data from unvaccinated populations, so it cannot determine if a vaccine caused something. Without a control (or comparison) group, we don’t know if the adverse events (including deaths) reported to VAERS are part of the background — that is, things we usually see, even before 2020.
After all, VAERS accepts reports regardless of whether they are likely or unlikely to be caused by the vaccines, and bad things — deaths, diseases, and illnesses — happen to people daily.
In 2019, 2.85 million people died in the U.S., which gives an average of 7,800 deaths per day. So, one can imagine if the most vulnerable populations are prioritized for vaccination at a massive scale, a drastic spike in post-vaccine adverse events and deaths will happen every day.
Even before the pandemic, about 10% and 12% of deaths in 18–64-year-olds and 9–39-year-olds, respectively, were unexplainable. So, in the context of mass vaccination, we have a candidate to blame for unexplainable deaths.
***
But if the spike in post-vaccine adverse events and deaths exceeded the background rate (i.e., what we normally see regardless of the pandemic), then it’s a signal that the vaccines could be dangerous.
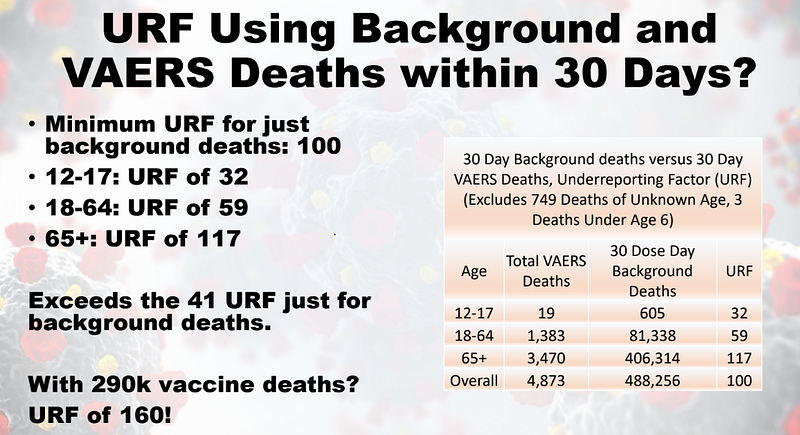
Did it exceed though? At least for deaths, it didn’t. Even with an underreporting factor of 41-times (as some have claimed, which may or may not be accurate as the underreporting factor differs between adverse events), it’s not enough to surpass the 30-day mortality background rate.
The post-vaccine deaths (within 30 days) have to be multiplied by 100-times just to reach the background rate of 30-day mortality. In other words, even with an underreporting factor of 100, there are no excess deaths in VAERS.
Speaking of excess deaths, it’s another metric to judge vaccine safety. Another author of this publication has compared excess deaths, Covid-19 deaths, and vaccination rates between countries, writing that:
“If the vaccine is highly lethal, it has to be highly lethal everywhere. Finding one country that had some excess deaths at the same time as vaccinations doesn’t prove the vaccine is deadly, because those deaths could also be from covid. But finding one country, where there was mass vaccination with no excess deaths is good proof that the vaccine is not deadly. I just pointed to 6 countries as proof.”
The author has also written another brilliant article on how VAERS is better understood. Matt Timberlake has also done the same in a presentation with Yuri Deigin that was posted as a Youtube video.
All that said, this section is not to dismiss VAERS reports/anecdotes entirely. We cannot completely rule out that the vaccines might have caused a fraction of the adverse events (including deaths) in VAERS. After all, the top three surveillance studies described above did find excess adverse events associated with the mRNA and DNA vaccines. But to conclude that vaccines are dangerous based on VAERS alone isn't fair.
Key points
As randomized controlled trials (RCTs) mainly included healthy adults, we aren’t very sure if the vaccine will behave the same in the real world, necessitating surveillance studies. At least six large-scale surveillance studies on Covid-19 vaccines have been published. Based on the top three ones I identified, the mRNA and DNA vaccines are associated with increased risks of several adverse events — such as stroke, blood clotting disorders, and Guillain-Barre syndrome — leading to several excess cases and deaths.
But this happened to the tiny minority. For example, based on the top three surveillance studies identified, the adverse event that produced the highest excess cases is ischaemic stroke from Pfizer’s mRNA vaccine — at 143 excess cases per 10 million people, with about a 15% death rate. But it also means that the remaining 9,999,857 people did not develop stroke after getting the vaccine. Thus, the Covid-19 vaccines are safe in the vast majority, much safer than Covid-19. But the tiny minority that the vaccines harmed is unfortunate, which may have led some to overestimate vaccine risks.
To close, the topic of vaccine safety is sophisticated and vast. So, I must admit that not every single argument on vaccine safety is covered in this article. I’m not writing a textbook after all. Lastly, I’m only one person, so I may have made mistakes or overlooked certain things. In the end, even this article should be regarded as approximate truth, not an absolute one.
If you have made it this far, thank you. Subscribe to my Medium email list here. If you want to become a member to get unlimited access to Medium, you can use my referral link, and I will receive a small commission at no extra cost to you. You can also tip me below if you are feeling generous today, and I’ll appreciate it. Paying bills with science writing isn’t easy, so I’ll appreciate any help I can get.





