
BLM in Women’s Health; Lack of Access to Healthcare Costs Lives
Racial inequities in pregnancy and breast cancer
America is on edge. The death of George Floyd poured accelerant on our inflamed society. Our highly polarized politics fan the simmering COVID-19 flames.
Police brutality and the need for criminal justice reform were prescient topics before Floyd’s death. He was not the first and sadly will not be last.
But in the current context, Floyd’s murder ignited widespread multiracial support for the Black Lives Matter Movement.
I am proud to be a part of the pluralistic support.
I am an Obstetrician-Gynecologist working in one of the most ethnically diverse American communities. Our patient population is socioeconomically, racially, and ethnically diverse. Our patients come from all over the world.
The multicultural nature of our practice population and the racial diversity of our medical providers provides me with a unique perspective on women’s health issues.
Yet, I am terrified to post this article.
As an affluent white man, who I am to speak out the issue of racial disparity? How will the message be received? Will I be accused of mansplaining, white fragility, grandstanding, liberal guilt, or be laughed at for suddenly recognizing racial disparity in our society?
Probably yes.
Critics are always present. As I struggled to click the “publish” icon, I remembered an article I wrote in January which reminded me of how to cope with critics.
The truth is, I can not help if I don't speak out.
I will never understand the deeper way black people experience racism.
But I want to.
Listening, learning, reading, and engaging are my tools to increase consciousness, but to make a significant difference I want to take action.
I can not and will not try to speak about what it’s like to be black. What I can speak to is the racial disparity for women of color in pregnancy and breast cancer.
For 21 years, I have provided obstetrical care to women in the Dallas/Fort Worth Metroplex. Obgyn’s deal with two health conditions every single day that illustrates a clear cut pattern of systemic bias.
The high mortality rate in black women due to pregnancy and breast cancer warrants society’s attention and increased public funding.
While the protests amplify systemic structural racism in our society, we can also highlight the racial disparities in healthcare. COVID-19 deaths and infection rates disproportionally affect black and Latino populations.
Former Vice President Joe Biden’s statement called out the racial inequities of the COVID-19 pandemic. “An early data analysis from the Washington Post indicates that counties with majority-Black populations have coronavirus infection rates three times higher than counties with majority white residents, with death rates nearly six times higher.”
Public policy experts blame the lack of health insurance access, preexisting conditions, environmental factors, and social habits. These factors serve as a high-level summary of the complex conglomeration of causes.
But these are recurrent themes. These same concepts apply to health scenarios beyond coronavirus.
Healthcare access is a repetitive factor. We see it over and over again making the lack of access to care a central issue in racial health disparity.

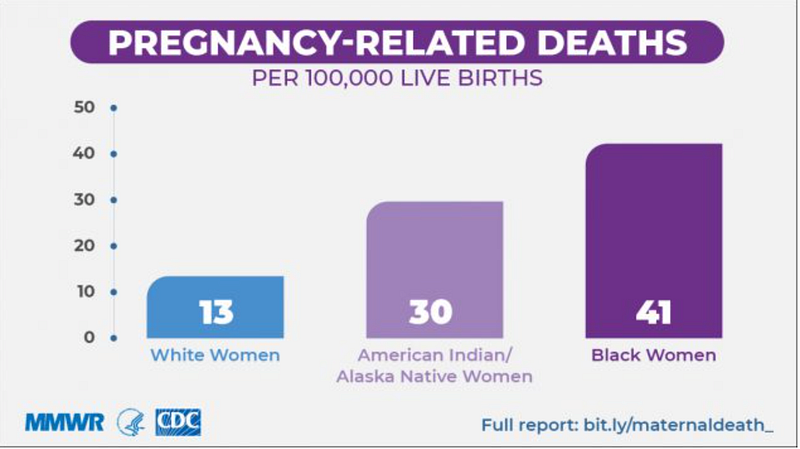
Maternal Mortality
The United States maternal mortality rate is the highest of any developed nation. We lose approximately 700 lives each year due to complications of pregnancy.
Black and other women of color are two to three times more likely to die from pregnancy-related causes than white women. This risk increases with age. For women over the age of 30, the risk of dying during or after pregnancy is four to five times higher than for white women.
Maternal mortality review committees in the CDC report 60 percent of maternal deaths are preventable.
Simplistic explanations do not justify these horrific statistics. The disparities remain true when controlling for socioeconomic status and lifestyle choices.
To be clear, poverty does not explain away the numbers.
My African-American partner speaking from her own experience, “I am an Obgyn and it is hard to stomach that no matter what, I am still at risk just because I am black.”
It is hard to emotionally and intellectually process her words. They sting.
But her statement is true. Socioeconomics does not explain away the numbers.
Kira Dixon Johnson’s story is gut-wrenching. Her husband’s words tell the story we all need to hear.
Women of color die at a 243% higher rate than white women regardless of education level and income status.
243%
To understand these numbers, we must acknowledge the complexity of the contributing multidimensional factors. Preexisting medical conditions, socioeconomics, cultural differences, and biological differences play a significant role. The standardization of medical care, bias, and racism are also factors.
But nothing contributes more than the lack of access to high-quality healthcare.
Given the compounding variables leading to the elevated maternal death rate in women of color, I will focus attention on my area of expertise: caring for women on Medicaid.
Preexisting chronic diseases such as obesity, hypertension, and diabetes are higher in women of color. Preconception disease optimization reduces risk.
For women without health insurance, managing preexisting medical conditions becomes a monumental task.
The 2010 Affordable Care Act (ACA) increased coverage in our country, but millions of Americans are still without health insurance.
The lack of access to high quality, affordable healthcare increases poor health outcomes and widens the racial disparities.
Why do pregnant women die?
- Cardiomyopathy and another cardiac disease
- Thrombotic pulmonary embolism
- Preeclampsia and hypertensive disorders of pregnancy
- Hemorrhage
- Cerebrovascular accidents (strokes)
- Infections

To address preexisting conditions, patients need access to medical providers. Primary care, Obgyn, and specialist care before, during, and after pregnancy, reduce the risk of death. Risks are identified, treated, and prevented.
Many Americans access the US Health system through the Medicaid program. Medicaid covers almost half of the births in our country. In my state, Texas, 54% of pregnant women qualify for Medicaid. But many states chose not to expand Medicaid under the provisions of the Affordable Care Act.
Federal law dictates states must provide prenatal coverage through the Medicaid program. Pregnant women with family incomes up to 138% of the federal poverty level qualify for mandatory coverage.
Medicaid coverage does not begin until the pregnant woman completes the pregnancy verification process. For many women, this process is slow and arduous. Federally mandated prenatal coverage also ends 60 days postpartum.
In the US, we provide Medicaid AFTER patients get pregnant and take it away when they deliver. Women gain temporary access to the US health system once they become pregnant and lose access once they deliver.
The Medicaid system sets up missed opportunities
Healthcare providers miss a critical opportunity to manage patients beyond the 60-day postpartum period. The 4th trimester is a crucial time for medical care considering one-third of the peripartum deaths occur in the first year after delivery.
If we can’t see the patient, then we can’t prevent these problems
Through the Medicaid qualification system, providers lose the opportunity for pre-conceptual counseling and pre-existing condition disease optimization. When patients qualify for Medicaid and arrive in our office late in pregnancy, Obgyn’s across the nation struggle playing catch up to manage chronic hypertension and diabetes.
Access to specialists in cardiology, endocrinology, nephrology, and hematology is often lacking or impossible for those on Medicaid. Knowing 31% of maternal deaths occur before labor and delivery, early intervention and prepregnancy disease management is a vital prevention tool.
Worsening the problem, states are not required to provide full Medicaid benefits under federal guidelines. States may provide limited coverage to only pregnancy-related services through a program called CHIP.
Obstetricians, certified nurse-midwives, and their patients are left with limited referral options for patients with the highest risks.
Maternity care deserts
Many areas of the United States lack basic maternity services. These areas are called maternity care deserts. If women can not physically get to a qualified obstetrical care provider’s office, then poor outcomes are expected.
Some hospitals are closing maternity units in states that did not expand under the Affordable Care Act. Fewer labor and delivery units result in a further reduction in obstetrical options and a reduction in access to care.
The problem may be getting worse.
In response to the increase in maternal deaths, states are implementing Maternal Designation programs. Large publically traded companies fund these programs. Company lobbyists work with state officials to implement policies requiring the services their companies provide.
Unfortunately, these well-intended maternal mortality reduction plans may inadvertently exacerbate the problem. Smaller and rural hospitals may close down more women’s services departments as they cannot meet newly imposed regulatory requirements.
Policymakers often equate maternity care desserts as a rural health issue. While remote geographic locations create logistical challenges, it is also true that large urban areas often lack doctors and hospitals who accept Medicaid insurance.
The low Medicaid reimbursement rate disincentivizes providers from taking on these patients. Nonprofit hospitals funded by taxpayer money often meet federal guidelines by contracting with traditional Medicaid, but avoid contracting with the various third party managed Medicaid plans pregnant patients are actually using.
The result: Pregnant women with Medicaid often can not find an in-network hospital facility or a medical provider who will see her.
Our national public policy sets up the process to fail. For Obstetricians who care for Medicaid patients, none of this information is new news.
As a society, we must recognize if we do not provide high-quality medical care before, during, and after pregnancy then we will suffer the consequences later.
The price is 700 new mommy’s lives each year.
The racial disparity goes beyond pregnancy
Maternal mortality is only one women’s health racial disparity issue. 38% of U.S. females identify as a racial or ethnic minority group and 50 % of US births were to women of color. People of color will represent most of the U.S. population by 2050.
As our country's demographic changes, we must recognize the racial disparity and implement public policy changes to address them.
Infant Mortality
African Americans have the highest infant mortality rate of any racial or ethnic group in the United States. This is mainly due to an elevated risk of preterm birth. Many Obstetricians have implemented specific prevention programs, but more research is needed to provide clear cut evidenced-based practice guidelines.
Screening patients for a history of preterm birth is one simple step women’s health providers can employ. Some may consider universal sonogram cervical length screening and increasing the use of preventative Progesterone therapy. More scientific research specific to black populations is needed to validate these steps.
More funding is needed to encourage more research. Reducing preterm birth rates will save infant lives.
Systemic changes in pediatric care can save lives and reduce the infant mortality rate. The same health access issues discussed in maternity care apply to newborn care.
Babies covered by Medicaid struggle to find high-quality pediatric offices accepting new patients.
Public policy must increase funding to the support system families require such as Medicaid, Children’s Health Insurance Program (CHIP), Temporary Assistance for Needy Families (TANF), and nutrition assistance programs.
Instead, our federal and state governments are cutting funding for all of these programs.
Society should care just as much about babies after delivery as they do when still in the uterus.

Breast Cancer
Although black women and white women get breast cancer at the same rate, the breast cancer death rate in black women is 40% higher than white women. Again, we come back to the problem of health care access.
Those without health insurance have less access to preventative screening, provider breast examinations, and mammography. Breast cancer in black women is often detected at a more advanced stage. Black women are also at higher risk of a particular type of breast cancer called TNBC.
Universal screening guidelines do not change based on race despite the evidence that black women develop breast cancer at a younger age. Black women under age 35 get breast cancer at twice the rate of white women.
Most insurance plans, Medicaid, and Medicare only cover screening mammography beginning at age 40.
Genetic screening is an additional tool to mitigate the racial disparity in breast cancer. Taking a family history identifies those who qualify for altered screening protocols and BRCA genetic testing.
Funding is needed for more medical research to determine why a particularly deadly type of breast cancer is twice as common in black women. Triple-negative breast cancer (TNBC) has less available treatments, spreads faster, and often is diagnosed at later stages.
Solving problems requires systemic changes
Pregnancy care and breast cancer are only two examples. Many other medical issues follow the same patterns. Each issue requires different strategies.
Simple solutions won't work.
Some racial disparities in health are directly linked to socioeconomic inequities such as income, housing, education, and job opportunities. But as a society, we must acknowledge the disparities don’t go away when we remove these compounding variables.
To save lives, the US health system must make decisions. Are we ready “to put our money where our mouth is” and provide scalable solutions?
We must acknowledge the racial disparity in healthcare. Identify solutions. Fund medical research. Implement strategies on a systemic level to solve problems.
We must also vote in elections to elect leaders willing to initiate change.
The challenge for us as leaders is ensuring support gets to those who need it immediately, and doing the necessary work to rip out the structural racism that creates these inequalities wherever we find it. Vice President Joe Biden