
What is MIMIC-IV? Newer, Better, Modular Release of MIMIC
When MIMIC-III becomes modular, release v2.2 Jan 2023
The Medical Information Mart for Intensive Care (MIMIC) database is a collection of patient data from intensive care units that can be used to improve patient care through knowledge discovery and algorithm development. MIMIC-III was deidentified to protect patient privacy and has been used in a lot of research in clinical informatics, epidemiology, and machine learning. Publication link
MIMIC-IV is an updated version that incorporates a modular approach to data organization. It highlights the data province and facilitates individual and combined use of the disparate data source. Its goal is to continue the success of MIMIC-III and support a wide range of healthcare applications.
MIMIC code-repository can be found here
How Large Is MIMIC-IV
The counts are as follows:
- patients: 299,712 (was 315,460 in v2.0) after removal of test data
- admissions: 431,231 (was 454,324 in v2.0) after removal of test data
- icustays: 73,181 (was 76,943 in v2.0) after removal of test data
How is MIMIC-IV built?
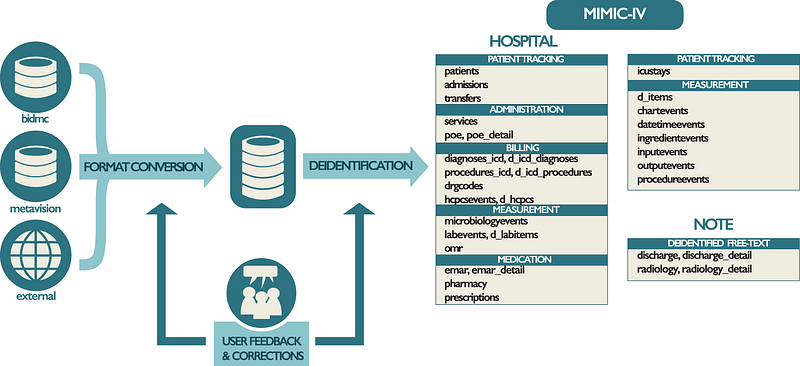
Overview of data processing in the MIMIC. Data are acquired from —
- the BIDMC data warehouse
- the ICU information system (MetaVision), and
- external sources (“acquisition”).
Structured Query Language (SQL) scripts merge the various data sources into a single schema (“transformation”). Finally, deidentification algorithms are applied to remove protected health information from the reformatted schema selectively. Tables present in MIMIC-IV are provided on the far right of the figure under their respective module. Issues raised on the MIMIC Code Repository are assessed and used to improve the build process as appropriate.
Data Acquisition
Source: Beth Israel Deaconess Medical Center (BIDMC) emergency department or one of the intensive care units
Admission years: 2008–2019

Data Preparation
The preparation step involved removing unnecessary content: denormalizing tables, removing audit trails, and reorganizing into fewer tables. However, no standardization or data cleaning was done at this step to preserve the raw information.
Data Deidentification
Structured data: HIPAA patient identifiers (PHI) were removed, and Patient identifiers were replaced using a random cipher, resulting in deidentified integer identifiers for patients, hospitalizations, and ICU stays. Freetext deidentification: MIMIC uses its own software package linked here.
Protected Health Information (PHI) (ref).
- Name
- Address (all geographic subdivisions smaller than state, including street address, city county, and zip code)
- All elements (except years) of dates related to an individual (including birthdate, admission date, discharge date, date of death, and exact age if over 89)
- Telephone numbers
- Fax number
- Email address
- Social Security Number
- Medical record number
- Health plan beneficiary number
- Account number
- Certificate or license number
- Vehicle identifiers and serial numbers, including license plate numbers
- Device identifiers and serial numbers
- Web URL
- Internet Protocol (IP) Address
- Finger or voice print
- Photographic image — Photographic images are not limited to images of the face.
- Any other characteristic that could uniquely identify the individual
Finally,
dates and times were shifted randomly into the future using an offset measured in days. A single date shift was assigned to each subject_id. As a result, the data for a single patient is internally consistent.
Modules
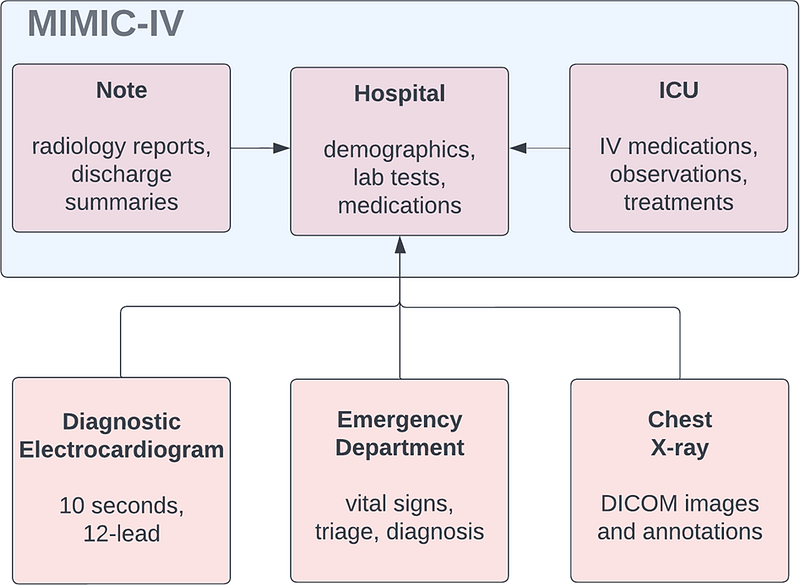
Hospital Module
The hosp module contains data derived from the hospital-wide EHR. These measurements are predominantly recorded during the hospital stay, though some tables include data from outside the hospital as well (e.g. outpatient laboratory tests in labevents).
- Information includes patient and admission details (patients, admissions, transfers) - Laboratory measurements (labevents, d_labitems) - Microbiology cultures (microbiology events) - Provider orders (poe, poe_detail) - Medication administration (emar, emar_detail) - Medication prescription (prescriptions, pharmacy) - Hospital billing information (diagnoses_icd, d_icd_diagnoses, procedures_icd, d_icd_procedures, hcpcsevents, d_hcpcs, drgcodes) - Hospital service related information (services)
ICU module
The ICU module contains data sourced from the clinical information system at the BIDMC: MetaVision (iMDSoft). MetaVision tables were denormalized to create a star schema where the icustays and d_items tables link to a set of data tables all suffixed with “events”. Data documented in the icu module includes
intravenous and fluid inputs (inputevents) ingredients of the aforementioned inputs (ingredientevents) patient outputs (outputevents) procedures (procedureevents) information documented as a date or time (datetimeevents) other charted information (chartevents). All events tables contain a stay_id column allowing identification of the associated ICU patient in icustays an itemid column allowing identification of the concept documented in d_items Contains one column: caregiver_id, a deidentified integer that uniquely represents a single caregiver or provider. These identifiers are sourced from the MetaVision ICU system. When present in a table, it indicates the user who documented the data into MetaVision. For example, the caregiver_id associated with a row indicating mechanical ventilation in the procedure events table represents the user who documented the event and not the provider who performed the procedure.
Emergency department Module
The ED module contains data for emergency department patients collected while in the ED. Information includes a reason for admission, triage assessment, vital signs, and medication reconciliation. The subject_id and hadm_id identifiers allow MIMIC-IV-ED to be linked to other MIMIC-IV modules.
CXR module
MIMIC-CXR contains 227,835 imaging studies for 64,588 patients presenting to the Beth Israel Deaconess Medical Center Emergency Department between 2011–2016. A total of 377,110 images are available in the dataset. Each imaging study can contain one or more images, usually a frontal view and a lateral view. Studies are made available with a semi-structured free-text radiology report that describes the radiological findings of the images, written by a practicing radiologist contemporaneously during routine clinical care. All images and reports have been de-identified to protect patient privacy.
A records file, cxr-record-list.csv.gz, provides a mapping between the image (dicom_id), the study (study_id), and the patient (subject_id). Another records file, cxr-study-list.csv.gz, provides a mapping between the studies (study_id) and patients (subject_id).
Images are provided in DICOM format; see the image section for more information about the images. Reports are provided as plain text files; see the reports section for more information about the reports.
Notes Module
This is the only module from MIMIC-IV that is not publicly available. It has information on patient discharge and radiology. It includes free-text summary of the discharge (also known as discharge-notes) and radiology reports. There is additional information about discharge and radiology (auxiliary information) available for research. Also, being a new module the structure of this module is yet to be determined. So we need to wait a bit for the final form.
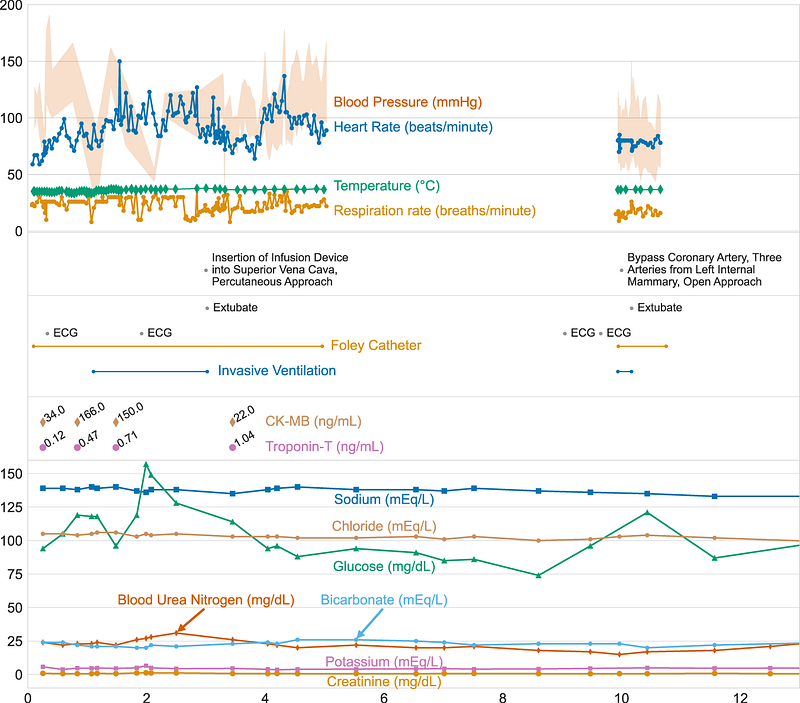
Data Visualized for a single patient
Here is how the data looks like when visualized for a single patients over time. Following table is generated from the MIMIC-IV data for patient with hadm_id =28503629.
Three vertically stacked panels highlight the variety of information available. Vital signs are shown in the top panel: note that the frequency of data collection for temperature is much higher at the start of the ICU stay due to targeted temperature management. Procedures from multiple sources are shown in the middle panel, including billing information, the provider order entry system, and the ICU information system. The bottom panel displays patient laboratory measurements. While frequent vital signs are only available when the patient is in the ICU, laboratory measures are available throughout their hospitalization.
How Can I Access MIMIC-IV?
Even though MIMIC-IV is unidentified, the dataset contains information about real patients. This information must be treated with care and respect. Hence, a few steps must be followed before one can access this data as follows —
- Become a credentialed user on PhysioNet. This involves the completion of a training course in human subjects research.
- Sign the data use agreement (DUA). Adherence to the terms of the DUA is paramount.
- Follow the tutorials for direct cloud access (recommended), or download the data locally.
Instructions specific to the CXR module
To access this module, you must sign the data use agreement for MIMIC-CXR and request access to MIMIC-CXR data on BigQuery via the MIMIC-CXR PhysioNet project page.
Terms of Usage (DUA)
To my readers from the non-healthcare industry. Please take time to read through all the terms. Healthcare is a different ball of wax when it comes to data science. We deal with real patient data day-in-and-day-out. Kindly do everything in your power to protect, care, and respect the information of fellow humans. Some day, in some datasets, your information will be treated the same.
The Terms of the DUA are as follows (MIMIC-III v 1.4 DUA). Unfortunately, the v2.2 (a release for MIMIC-IV) specific DUA is not available on the website. I am guessing that MIMIc-III DUA has not changed and is still in use. I have emailed to physionet. Upon getting a response, I will update the article accordingly. Until then, here are the terms of the DUA.
If I am granted access to the database:
- I will not attempt to identify any individual or institution referenced in PhysioNet-restricted data.
- I will exercise all reasonable and prudent care to avoid disclosure of the identity of any individual or institution referenced in PhysioNet restricted data in any publication or other communication.
- I will not share access to PhysioNet restricted data with anyone else.
- I will exercise all reasonable and prudent care to maintain the physical and electronic security of PhysioNet restricted data.
- If I find information within PhysioNet restricted data that I believe might permit identification of any individual or institution, I will report the location of this information promptly by email to [email protected], citing the location of the specific information in question.
- I have requested access to PhysioNet restricted data for the sole purpose of lawful use in scientific research, and I will use my privilege of access, if it is granted, for this purpose and no other.
- I have completed a training program in human research subject protections and HIPAA regulations, and I am submitting proof of having done so.
- I will indicate the general purpose for which I intend to use the database in my application.
- If I openly disseminate my results, I will also contribute the code used to produce those results to a repository that is open to the research community.
- This agreement may be terminated by either party at any time, but my obligations with respect to PhysioNet data shall continue after termination.
Guidelines For Users
MIMIC-IV data usage for research comes with a specific set of guidelines.
- Specify the version of MIMIC used in the study, such as MIMIC-III v1.4 or MIMIC-IV v1.0, and provide a reason if an older version is used.
- Distinguish clearly between ICU and hospital admissions in the study.
- Be specific about the definition of mortality used, as it can be defined in various ways. It is recommended to use 30-day mortality from ICU admission as it reflects the patient’s illness severity at admission.
- Use clear and specific criteria for patient selection and exclusion rather than vague terms.
- Include a proper citation for the MIMIC data and for MIMIC-III; also cite the corresponding paper. Check the acknowledgment page for more details.
Conclusion
MIMIC-IV is a step in the right direction for promoting research for healthcare. However, being only limited to emergency visits, the corpus is restricted in many ways. More efforts and investments are necessary to develop de-identified and publicly available healthcare records to allow a wider set of researchers from various backgrounds to explore. Invariably, such efforts will lead to better research in the long term.

To support me 🔔 clap | follow | Subscribe 🔔
Become a member using my link: https://ithinkbot.com/membership
Checkout my other works —