
The Volunteers who Challenge the Virus: Controlled Human Infections
Would you be a volunteer who challenges the virus?

In a time where everybody tries to protect themselves from COVID-19 — by wearing masks, respecting social distancing, or avoiding shared surfaces — some are facing the virus head-on!
Yes, thousands of people have expressed interest in participating in Controlled Human Infection (CHI) studies with SARS-CoV-2, the causative agent of COVID-19.
CHI studies aim to speed up the development of a vaccine for COVID-19. According to 1daysooner.org, a website that encourages people to volunteer to participate in human challenge trials or to advocate on their behalf, almost 30000 people from 140 countries have already applied to deliberately expose themselves to SARS-CoV-2. This is surprising, given that COVID-19 is like the “perfect” pandemic, it killed almost 500000 people worldwide and no specific treatments are available.
Why do these volunteers want to take on a life-threatening risk?
There are multiple reasons: some have strong motivations to help others, some people are motivated by the money while other volunteers are curious of the experience.
The perspective of one 41-year-old volunteer is very interesting, as the owner of a business that has him visiting warehouses and flying regularly, he figures he’ll inevitably get infected anyways, so he declared on CNN: “I feel if I did it under a controlled environment, and I had an adverse reaction, my chances are much better”.
On one hand, Dr. Lipsitch, a Harvard epidemiologist, confirmed that “as a part of being in the trial they [partecipants] would be guaranteed excellent care if they needed it”. On the other hand, controlled human infection studies continue to generate controversy within the scientific community especially from an ethical point of view. It may seem impermissible to ask people to take on the risk of severe illness or death, even for an important collective gain.
To better understand the scientific doubts on this matter let’s start by defining controlled human infection studies.
In CHI studies, a small number of healthy participants are deliberately exposed to a known dose of a pathogen in a controlled setting, to study infection and gather preliminary efficacy data on experimental vaccines or treatments.
CHI studies, by allowing preliminary efficacy testing in 10–100 participants, are cheaper than phase 2 and 3 clinical trials that often require sample sizes ranging from hundreds to hundreds of thousands of participants. Thus, they help to identify inferior vaccine candidates or treatments before initiating large safety and efficacy trials, allowing valuable resources to be focused on those candidates that have the greatest potential for success.
CHI studies have emerged as powerful tools to select promising new vaccines or drugs on the increasingly complex and expensive path towards licensure. In this decade more than 120 controlled human infection studies have been published, primarily for influenza, rhinovirus, typhoid and malaria.
A malaria CHI study provided critical information for the development of the malaria vaccine RTS,S. Malaria CHI studies were performed to first evaluate the efficacy of this vaccine and to then further refine the formulation and dosing regimen before initiating Phase 3 efficacy evaluations in Africa. A dengue CHI study was used to determine which formulation of a live-attenuated tetravalent dengue vaccine should be chosen to move forward in a Phase 3 efficacy trial in Brazil.
The CHI approach calls to mind the case of Dr. Barry J. Marshall who won, together with J. Robin Warren, the 2005 Nobel Prize for Physiology or Medicine for their discovery of “the bacterium Helicobacter pylori and its role in gastritis and peptic ulcer disease“.
Unable to make his case in studies with lab mice (because Helicobacter pylori affects only primates) and prohibited from experimenting on people, Marshall grew desperate. Finally, he ran an experiment on the only human patient he could ethically recruit: himself!
He took some Helicobacter pylori from the gut of an ailing patient, stirred it into a broth, and drank it. He developed gastritis and later an ulcer, thus, he biopsied his own gut, culturing Helicobacter pylori and proving unequivocally that bacteria were the underlying cause of ulcers.
Marshall’s experiment could be thought of as the “father” of CHI studies, while on the other hand the sodium-bicarbonate drinks (enriched with the pathogen) used to infect volunteers during CHI studies for typhoid vaccine seem to be the worthy heirs of Marshall’s broth!

Despite their invaluable contribution to science and product development, the demanding nature of CHI trials and the risks involved require careful risk-benefit assessments.
It is clear that SARS-CoV-2 CHIs have high social value:
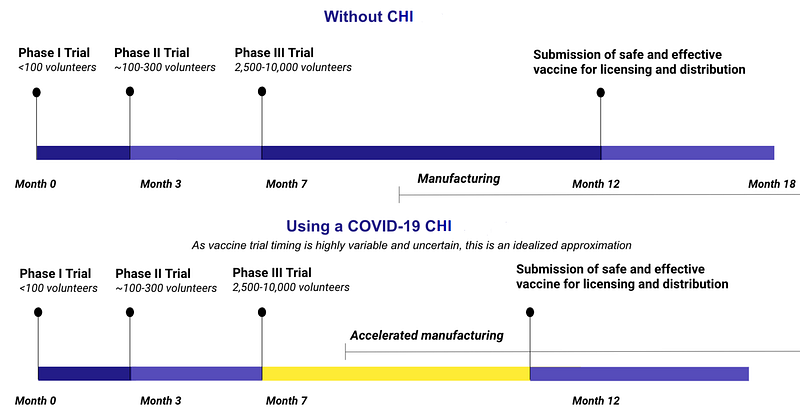
1. they could help identify the most promising vaccine against COVID-19 and accelerate product development (see figure below);
2. by saving time -even a few months- in vaccine development they would contribute to faster control of the pandemic -mitigating both economic and social costs of emergency measures;
3. they could address multiple scientific questions: dynamics of infection, viral pathogenesis, how infections occurred, identify correlates of immune protection.
However, even if CHI studies have high social value, the safety of participants is a primary concern at all times. To be recognized as ethically permissible, the risk to CHI participants should not exceed an absolute upper limit of 1% mortality risk.
To minimize risks to participants, SARS-CoV-2 CHIs recruit young people without underlying medical conditions because they face lower mortality risks from COVID-19. In fact, current data suggest that 20- to 44-year-olds with diagnosed infection — including those with underlying conditions — have a mortality risk of less than 0.2%. The presence of asymptomatic people further reduces the predicted fatality rate. In those aged 18–30 years (whether healthy or not), hospitalization rates for COVID-19 are currently estimated to be around 1% and fatal infection rates around 0.03%. Thus, fair participant selection would seem sufficient to ensure that risks from SARS-CoV-2 CHIs remain well below the ethically acceptable limit.
What is the ethical controversy of SARS-CoV-2 CHIs?
Dr. Myron Levine, associate dean for global health, vaccinology, and infectious diseases at the University of Maryland brings us to the heart of the matter: “I think one needs to have therapy before one would undertake a challenge”. Dr. Levine has conducted CHIs for decades studying cholera, shigella, malaria but he argued that without an efficient treatment to cure any volunteers who might go on to develop severe illness in a trial, a CHI study cannot be conducted.
Although treatment is one important way of reducing risk, the existence of specific, curative treatments is not a necessary condition for the ethical acceptability of challenge studies.
But it is also true that key uncertainties remain regarding potentially serious and irreversible harms of SARS-CoV-2 infection in young people, such as cardiac or neurological injury. Pathogenesis of COVID-19 is currently poorly understood and it is not yet known why around 15% of patients contract the severe form of the disease.
If you are changing your opinion about CHI ethics you should also consider the fact that some participants would receive placebo vaccines, and that, probably, the majority of investigational vaccines would be ineffective.
There are thus strong motivations to conduct such studies especially carefully and to provide participants with high-quality supportive care (including intensive care if required), long-term follow-up (for any lasting harm), and full compensation for any harms that occur.
Participant selection is crucial and the informed consent processes are probably the key steps: the volunteers are faced with the risks and probably in this circumstance they make the real and ultimate choice — which should not be driven by economic compensation-.
Dr. Robert Read, head of clinical and experimental sciences at the University of Southampton, said: “You do have to be able to describe what you know of what could happen to them if they undertake a controlled infection, with complete clarity and honesty” — Probably, in the case of COVID-19, the matter of concern is what we still don’t know about SARS-CoV-2 —
Rigorous procedures to maximize participant understanding are required, CHI studies routinely incorporate tests of participant understanding during the informed consent.
“I think lots of volunteers, when faced with the information, would probably not consent to it” said Dr. Read.
What about you, would you give your consent, would you be a volunteer who challenges the virus?





