
The One Number You Need to Know If You Have Congestive Heart Failure
Your quality of life and how long you may live is a consequence of the “ejection fraction.”
During my more than 30 years as a cardiologist, I have diagnosed and treated thousands of patients with heart failure. As is standard medical practice, I took a detailed history, did a physical exam, and reviewed available data, such as an electrocardiogram, Chest X-ray, and blood work. In most instances, this was enough for me to establish a diagnosis. Yet, there is more that can be learned with advanced testing.
For decades, we have also been able to quantify the severity of heart failure. One cornerstone test, the echocardiogram, is an ultrasound of the heart. This measures the degree of impaired heart function.
Why do this?
The answer is that doing so allowed me to tailor-prescribe a treatment plan and afford the patient and their family a prognosis of how long they might live.
{kind=link}
Approximately 6.7 million adults in America have heart failure. The heart's sole purpose is to pump blood out to the body. When its ability to pump starts to fail, that is called heart failure.
At first, the symptoms could be subtle: weakness, fatigue, swollen ankles, or a cough. But as it progresses to congestive heart failure, usually shortness of breath at rest or with minimal activity ensues.
Again, the heart's sole purpose is to function as a pump. Its muscles and inherent electrical activity do this. If the heart muscle becomes diseased, it cannot pump efficiently. It still accepts blood, but because it can’t pump it out as strong or fast as before, it enlarges, and the blood, and therefore fluids it contains, backs up into the lungs.
The lungs are supposed to be filled with air and not fluid. When the latter happens, the result is congestive heart failure.
{kind=link}
Basic Heart Physiology
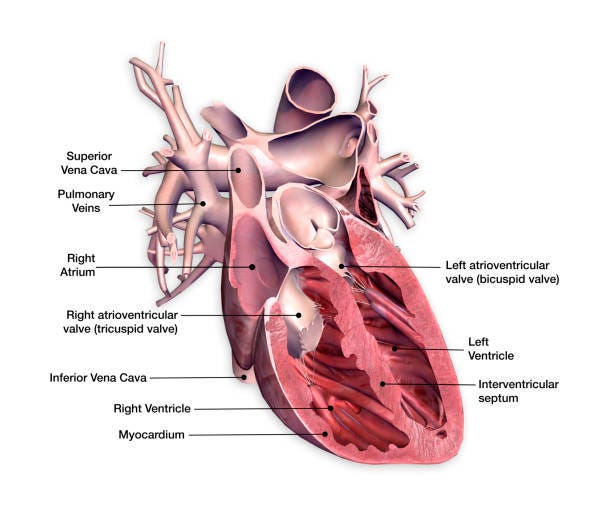
How our organs work is called physiology. The physiology of the heart is simple. There are four chambers: two upper ones on the left, called atria, and two on the right, named ventricles.
The right atria accept blood from the veins and are low on oxygen since our organs have extracted it as the blood circulates. After an electrical heart signal, the blood moves into another holding chamber, the right ventricle. After a brief pause to fill it up, the right ventricle pumps the blood to the lungs, where it picks up oxygen.
The newly oxygenated blood then fills the left atrium, pauses, and is dumped into the left ventricle. At another pause, the left ventricle pumps blood to the whole body, and the process repeats. Both atria beat and relax at the same time, and both ventricles behave similarly and in unison.
This cycle occurs 60 beats per minute, 86,400 times a day and 31,536,000 times yearly.
Congestive Heart Failure
When filled, the normally functioning human left ventricle will pump out or eject 55–70% of the blood it holds. This number is called the heart’s ejection fraction (EF). Any number less than 55% signals a high risk for congestive heart failure (CHF) or heart failure (HF) in the future.
The lower the number, the sooner HF is likely to develop, the worse it will be, and the shorter one’s life span.
Multiple studies show that the lower the ejection fraction, the greater one’s risk of dying in one, three, and five years. As an example, if you have HF and a low EF of 35–45%, you have a one in four chance of dying within three years.
If that number is 25–34%, that risk of dying increases to one in three. If the EF is reduced by less than 15%, that risk increases to more than one in two.
Risks of Heart Failure (HF) with a Normal Ejection Fraction (EF)
This is where things get more complicated. It has been noted that many HF patients have their disease despite a normal EF. This happens when a given disease causes the heart muscle to not relax properly during the resting or nonpumping phase of the heartbeat.
This relaxation phase is called diastole. The heart pumps out a normal amount of blood, but by not relaxing normally, the incoming blood to the ventricles cannot adequately fill that chamber. Then, backward pressure and heart failure may ensue.
Studies now show the mortality with HFpEF (Heart Failure with preserved EF) is almost as bad as HFrEF (Heart Failure with reduced EF). Almost half of HF patients have normal EF numbers. However, their mortality numbers are not as bad compared with patients who have HF with low EF’s.
Improvements in HF treatments
There have been improvements in HF treatments. However, morbidity and mortality remain high worldwide. Newer drugs, cardiac transplantation, and placement of dual ventricle pacemakers have helped somewhat. Pumping assist devices may be used as well, but are expensive, cumbersome, and not without risks.
What about a super-normal EF?
Having a very high EF can be a problem, too.
Studies have shown that HF patients with an EF of >70% have a similar mortality to those with a low EF of 35–45%. Again, the cause seems to be severe impairment of the heart’s ability to relax during diastole.
A new drug, Mavacamte, for treating this unique disease is now available. It is too soon to tell how it will improve overall mortality until its use becomes more common.
Takeaways
- CHF or HF is a very common disease in the US and worldwide. The mortality correlates linearly with how poorly the heart is pumping.
- The number to know is the ejection fraction or EF. The risk of dying within three years is inversely related to the EF. Thus, the lower the EF, the greater the risk of dying within a few years.
- HF patients with normal EF can also have limited longevity but, in general, is not as lethal as patients with low EF’s.
- The mortality has improved with newer treatments but still remains high.
- A “super-normal” EF can also cause higher mortality but not as bad as a lower EF. A new drug, Mavacamten, shows some promise.
If you, or a loved one, has HF, knowing your EF is important as it relates to mortality. However, many other factors are at play here, and even HF with a normal EF can reduce your chances of living three years or longer.
If given the choice, and we are not, it is better to have a normal rather than a very low EF.
Thank you for reading my story. I wish you a healthy life.
I am a retired MD passionate about culture, health, sports, and food. Get an email whenever I publish by clicking the below link: