
The Lies You’ve Been Told About Your Pain
Well meaning people may have given you bad information, and inadvertently made your pain worse.
I never thought very deeply about pain before I decided to return to university. I had experienced plenty of pain myself and seen other people in various types of physical and emotional pain, but I had not researched pain or had more than a superficial overview as part of an undergraduate biology course.
We were taught several different theories about pain as part of my schooling. Most popular among some of my professors was the gate control theory of pain.
Gate control theory asserts that activation of nerves which do not transmit pain signals, called non-nociceptive fibers, can interfere with signals from pain fibers, thereby inhibiting pain.
In other words, if you get punched in the arm, rubbing it feels good because you are interfering with the pain signal by activating normal touch receptors close to the site of injury. The gate theory is useful because it provides a sound physical and psychological model of pain, but it does fail to account for some aspects of the pain process.

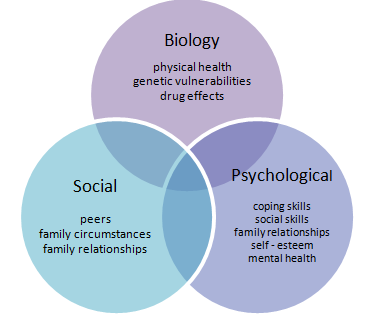
Biopsychosocial Model
The gate model of pain was one of the first to incorporate the mind and body in order to explain the pain process.
Today, there is much more known about the different types and functions of receptors, such that mechanoreceptors respond to touch and pressure, while thermoreceptors activate in response to changes in temperature. Nociceptors are associated with pain perception and, depending on the specific fiber (A, d or C) of the nociceptor type (mechanical, thermo-mechanical, or polymodal) that is stimulated, the perception of pain can range from sharp and prickly, to burning or freezing¹.
However, pain is complex and while models which address physiology and psychological interplay go part of the way to describing pain, they miss key components of painful experiences.
The biopsychosocial method of explaining pain takes more aspects of a person’s whole experience into account when addressing their pain. It recognizes that beyond physical injury and the central nervous system’s processing of tissue damage, lies a set of unique past experiences, social factors, and mental states which can prolong or delay the healing process.
For example, you may sprain your knee, which can lead to inactivity and muscle loss. Your doctor may even tell you to “go easy, maybe don’t go jogging for a while.”
Now you start to avoid jogging daily with your friend, which leads to being depressed about your loss of social interaction. Exercise and social interaction have analgesic effects, so now your pain may be worse even though you are doing what you think is right to allow the knee to heal. The knee heals fine, but maybe you have developed some fear or apprehension around jogging, worried that if you start jogging again the pain will return. This cycle of fear and avoidance can then have the potential to perpetuate pain and turn an acute injury into a chronic painful condition.
Untruth — Pain is in Your Brain
This is almost a mantra among a certain set of professionals who deal with people in pain, and I’ve used the expression myself in the office. An example I’ll give a patient that many of us have experienced is a paper cut.
You may have had the experience of cutting yourself on a piece of paper and not realizing it until you see the thin line of blood on your finger or hand.
All of a sudden, this small wound is extremely painful, painful WAY beyond the amount of tissue damage that has actually occurred. A good chunk of this pain is “in your brain” because the feeling of pain you are experiencing is disproportionate to the injury or threat you have received.
Another example would be a bruise, black and blue, on your arm or elsewhere. It’s fairly new but you have not noticed it and can’t remember what caused it. Did your sister’s dog jump on you the other day? Who knows, but you don’t remember anything painful happening at the time. Now you’ve finally seen the bruise, and all of a sudden, you are aware that it is painful.
Why wasn’t it painful before you noticed it?
If you’re otherwise occupied when something painful happens to you, you may not register it. This can happen with paper cuts and other trauma. When the mind finally gets around to it, the pain starts. So you might think then that pain is in your brain, and you’d be partly right.
Are you telling me it’s all in my head?
No.
If you take the position that pain is a function of your brain’s actions, then how can you reassert yourself to overcome your pain? If the brain alone dictates that you will have pain, what should be done to ease suffering?
The biopsychosocial approach to pain offers a more holistic approach.
After all, two different people who fracture their right wrist can have vastly different experiences of pain.
Person One may be in her 70s and have arthritis, diabetes, or some other previous illness predisposing them to longer recovery or chronicity. This woman may be retired and have plenty of time to come to her physical therapy sessions.
Person Two may be a 30 something smoker with poor sleep patterns who will not heal optimally either, but also cannot afford any time off from work to attend to rehab of the broken wrist.
Neither scenario is ideal for proper healing, and both patients undoubtedly felt a great deal of pain upon fracturing their wrists. However, each person is dealing with a complex interplay of biology, psychology, and social webs which will affect wound healing.
Different Strokes
While one patient may do well with some reassurance, a wrist splint, and a brochure on care at home, this approach will not suffice for another patient who has a social history of being in an abusive relationship where her partner grabbed her and fractured her wrist.
A healthy middle class athletic teenager from suburbia is going to experience pain differently than a refugee in a camp on some border fleeing conflict which has just killed or maimed half his family.
Stark examples but hopefully illustrative that pain is not merely a phenomenon of the brain, and care must taken when assessing past medical and social histories, and devising treatment plans. While the diagnoses may be the same, people’s ways in which pain is processed can vary considerably and will be affected by their environment, social circles, family dynamics, genetics, and a host of other factors.
Because two patients with the same diagnosis differ in physical, social, and psychological compositions, “lumping” these patients into the same treatment program will not likely produce the best outcomes compared to a tailored treatment regimen².
No two people will experience pain the same way.
Be careful of advice about pain which sounds good but may actually make your situation worse. You may be instructed to avoid certain activities, to rest, rely on passive interventions only (massage, hot packs, and other modalities that are done to you, without your active participation). People may mean well, but still contribute to you feeling worse in the long run.
If you enjoyed this article you may also like:
References:
- Basbaum AI and Jessell TM. The perception of pain. In: Kandel ER, Schwartz JH, Jessell TM, eds. Principles of Neural Science. McGraw Hill Companies. New York. 2000. pp 472–491.
- Gatchel RJ. Clinical Essentials of Pain Management. American Psychological Association. Washington, DC. 2005.