
The Diet-Cancer Connection
Investigating the influence of cruciferous vegetable, fiber, resistant starch, red meat, and organic food intake on cancer risk

While cancer is an umbrella term for a number of different diseases, cancers nonetheless share certain hallmarks, such as resistance to cell death, sustained proliferative signaling, and reprogramming of energy metabolism. To begin, let us examine one trait in particular: acquired resistance to apoptosis. Under normal conditions, cells that fail to pass certain cell checkpoints during mitosis, or cell division, are marked for programmed cell death via apoptosis, a form of cellular suicide. Cells that die in this manner slowly shrink and leave surrounding tissue intact (“not with a bang but a whimper”), and countless functional studies demonstrate that apoptosis serves as a natural barrier to cancer development. Similarly, suppression of apoptosis promotes tumor growth.
In contrast to apoptosis, necrosis involves lysis, or rupture, of the dying cell and the subsequent release of proinflammatory cytokines into the surrounding tissue microenvironment, akin to a supernova explosion. Necrotic cells recruit inflammatory immune cells to the site of damage, which can be actively tumor promoting since many such cells are capable of angiogenesis, the formation of new blood vessels. In this manner, necrotic cell death enables tumor growth by recruiting inflammatory cells that bring growth-stimulating factors to the surviving cells.
The tumor microenvironment is composed of surrounding noncancerous cells and molecules, which are often cajoled by cancer into acting as accomplices. If a given microenvironment was characterized by apoptosis as the dominant form of cell death over necrosis, that microenvironment could preclude the development of cancer. If cancer is not caused by mutations and dependent on the tumor microenvironment, how can an individual’s macroenvironment impact cellular microenvironments? Can dietary choices help maintain appropriate levels of apoptosis?
Can consumption of cruciferous vegetables lower cancer risk?
Cruciferous vegetables contain several compounds, including sulforaphane, that are capable of inducing apoptosis in breast, brain, blood, bone, colon, gastric, liver, lung, oral, ovarian, pancreatic, prostate, and skin cancer lines. Additionally, sulforaphane, found in broccoli sprouts, bok choy, and cabbage, also induces apoptosis in acute lymphoblastic leukemia (ALL), the most common blood cancer in children.
A 2008 study found that consumption of raw broccoli resulted in “faster absorption, higher bioavailability, and higher peak plasma amounts of sulforaphane” than consumption of cooked broccoli. Boiling, steaming, or microwaving at high power (850–900 watts) can inactivate a plant’s myrosinase content, which is necessary to break down glucosinolates, such as glucoraphanin (GR), into isothiocyanates (ITCs), such as sulforaphane (SF).
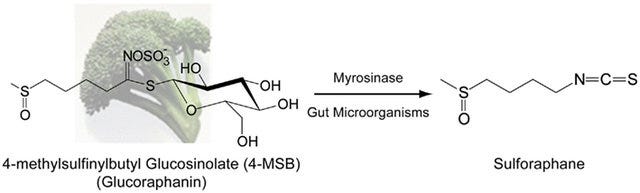
If eating raw vegetables is too hard to stomach, adding powdered brown mustard seeds, a rich source of myrosinase, to cooked broccoli also significantly increases the bioavailability of sulforaphane over that of cooked broccoli alone. Furthermore, while cooking denatures endogenous plant myrosinase, human colonic microbiota also possess myrosinase enzymes that can facilitate the hydrolysis of glucoraphanin to sulforaphane, albeit to a lesser extent than would occur in the small intestine.
Can consumption of resistant starch prevent colorectal cancer?
Colon cancer is the third most common type of cancer in the Western world and remains the third leading cause of cancer death in the United States. Particularly concerning is the recent rise of colon cancer among young adults. In 1973, Alan Berg observed that immigrants experienced an increased risk of colon cancer after moving to developed countries and converting to a Western diet.
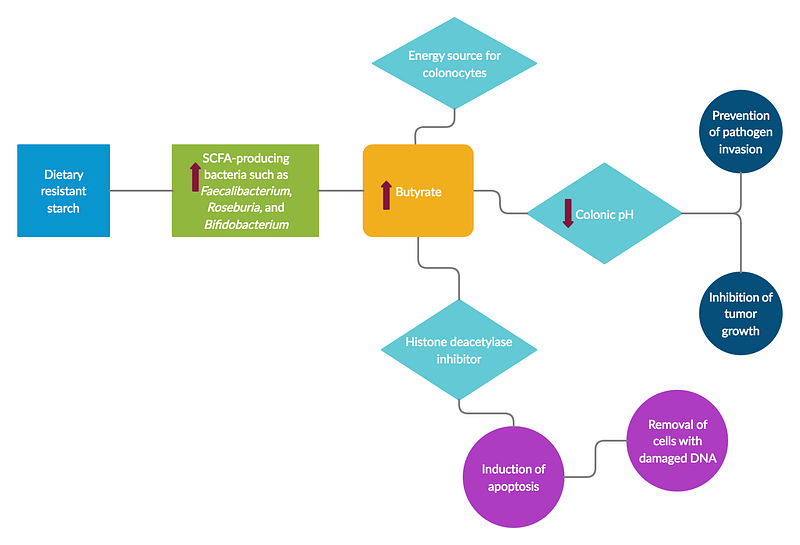
Native South Africans have some of the lowest colorectal cancer rates and often consume a diet rich in fermented, whole grain-maize porridge, which is oftentimes allowed to sit outside for several days after being made. These types of foods tend to be very high in a type of fiber known as resistant starch, which certain types of gut bacteria such as Faecalibacterium and Roseburia can ferment to produce butyrate, a short-chain fatty acid that promotes apoptosis and exerts a wide range of other anti-inflammatory effects.
Butyrate serves as the primary energy source for the colonic epithelium, lowers luminal pH, and helps prevent the development of tumorigenic colonic cell populations. Indeed, studies show that the gut microbiota of colorectal cancer patients are characterized by significantly lower numbers of butyrate-producing bacteria compared to healthy controls. Butyrate is a potent inhibitor of a class of enzymes known as histone deacetylases (HDACs), which relax chromatin structure and thereby enable the expression of genes that facilitate cell death and apoptosis. Murine models have shown that butyrate produced in response to resistant starch intake can inhibit colorectal carcinogenesis by enhancing the acute apoptotic response to genotoxic carcinogens. As Richard Le Leu of Flinders University of South Australia summarizes,
“Changes in amount of [dietary] fermentable substrate are capable of changing the biological response to DNA damage.”
Food exchange studies between Native Africans and African Americans have shown rapid reciprocal changes in the levels of bacteria responsible for sulfide production and those responsible for butyrate production. At baseline, the gut microbiota of Native Africans were characterized by higher numbers of starch degraders and butyrate producers while African Americans harbored higher numbers of potentially pathogenic Proteobacteria.
When African Americans switched to a Native African diet high in resistant starch and low in fat, butyrogenesis increased and colonic inflammation fell below the Native African baseline. The intervention diet consisted of hi-maize products, okra, lentils, rice, navy bean soup, mango slices, guava juice, samp, and other high-fiber foods. Conversely, Native Africans exhibited increased mucosal epithelial proliferation rates and colonic inflammation above the African American baseline upon switching to a Western diet of sausage links, hamburgers, French fries, meatloaf, Salisbury steak, noodles, corned beef hash, mashed potatoes & gravy, fried liver & onions, baked beans, and biscuits.
Not all fiber is created equal.

In contrast to other types of fiber such as non-starch polysaccharides (NSP), resistant starch may confer unique benefits. Resistant starch (RS) refers to starch that is not absorbed in the small intestine and reaches the colon undigested where it may be fermented by gut microbiota to produce short-chain fatty acids such as butyrate. RS may be characterized into five types, the first three of which occur in a normal human diet:
· RS1 describes starch that is physically trapped within plant cell walls and protein matrices and includes whole grains, seeds, and legumes
· RS2 consists of native, granular starch and includes green bananas, raw potatoes, and high amylose corn starch
· RS3 comprises retrograded starches that are formed when starchy foods (e.g. rice, potatoes, pasta, bread, cornflakes) are cooked and cooled
· RS4 is composed of chemically modified starches used in the food industry to commercially produce baked goods
· RS5 usually refers to amylose-lipid complexes, consisting of starch and fatty acids, that form during food processing, which may include the use of emulsifiers
Currently, daily intake recommendations for resistant starch have not been established, nor is RS content reported on food composition labels. The latter may be difficult to estimate given the various factors that can affect RS concentrations, such as ripening, natural variation, and cooking and storage methods. Clinical trials studying the influence of resistant starch intake on cancer risk must consider both the type of resistant starch used as well as the dose.
Approximately 20 grams of resistant starch intake per day may be necessary to confer digestive health benefits while intakes of 6 to 12 grams of resistant starch per meal have been observed to inhibit postprandial increases in blood glucose and blood insulin. Americans are estimated to consume about 4.9 grams of resistant starch per day, slightly below the range needed to observe beneficial effects at a single meal and considerably short of the daily intake associated with health benefits.
Lack of dietary RS3 may explain why colorectal cancer more commonly occurs in the distal colon rather than the proximal colon.
Most types of fiber consumed in a typical Western diet primarily ferment in the proximal portion of the colon. The proximal colon is connected to the small intestine by the cecum while the distal end of the colon is near the rectum. As previously mentioned, colorectal cancer is characterized by a reduction in butyrogenic bacteria in the gut. Among the different types of resistant starch, RS3 may be of particular importance for butyrate production, especially when combined with RS2.
RS2, such as raw potato starch, is granular, ferments quickly in the proximal part of the colon, and doesn’t change stool pH. On the other hand, RS3 is more crystalline, ferments slowly all the way to the distal end of the colon, and feeds SCFA-producing bacteria, thereby lowering colonic pH, preventing pathogen invasion, maintaining epithelial tissue health, and inhibiting carcinogenesis. A South African population consuming high levels of retrograded RS3 and low levels of dietary fiber was found to have significantly lower rates of colorectal cancer compared to another South African population that consumed higher levels of dietary fiber but lower levels of RS3; researchers speculated that RS3 fermentation was likely responsible for the observed protection.
A study examining the effects of resistant starch using human gut microbiota cultures found that RS3 doubled the proportion of Bifidobacteria in the distal colon and induced higher levels of butyrate production. The most common example of RS3 is cooked and cooled rice and potatoes, but green plantains, cassava, and taro also contain mixtures of several types of resistant starch, including RS3. A study examining the effects of resistant starch on several endpoints found that a high-RS diet produced a significant drop in fecal pH compared to a low-RS diet. The authors expound,
Fecal pH can be lowered by a variety of changes in the diet. Acid fecal pH has been linked with protection against bowel cancer. Epidemiological evidence suggests that a drop in pH by 0.5 units is associated with reduced risk. During this study we were able to reduce fecal pH by 0.6 units. To our knowledge, this is one of the largest diet-induced changes in human fecal pH reported. Studies using lactulose and oat bran have recorded decreases of 0.4 units. The results obtained here are most likely due to the higher amounts of [mixed] RS used because there was a significant inverse correlation between RS intake and pH, and between fecal starch and pH. In humans the majority of colon tumors occur in the distal colon. Thus, the measurement of fermentation-dependent events in feces may reflect the environment in the distal colon, and provide useful predictors of the antineoplastic properties of certain diets.
Does consumption of red meat increase the risk of developing colorectal cancer?
Over the years, a number of epidemiological studies have found correlations between red meat consumption and colorectal cancer, but a meta-analysis examining 35 of these prospective studies found the associations very weak in magnitude and not statistically significant. Additionally, red meat intake was generally more strongly associated with cancers of the distal colon than the proximal colon. Considering the fact that fermentation and SCFA production are greatest in the proximal colon with butyrate concentrations being inversely correlated to cancer risk, this particular finding may be less reflective of the influence of red meat on cancer risk and more indicative of the significance of intestinal microenvironments.
Observational studies also suffer from “healthy user bias,” which posits that individuals who engage in one behavior regarded as healthy likely also engage in other behaviors deemed healthy and vice versa. Consumption of red meat is also correlated with other potentially harmful behaviors such as alcohol consumption, smoking, lack of physical exercise, and low intake of vegetables. These confounding factors complicate our efforts to examine the impact of red meat intake in isolation. As Dr. Rachel R. Huxley at the La Trobe University in Australia summarizes,
“Given the frequent co-occurrence of smoking, alcohol, physical inactivity and diets that are high in meat (both processed and nonprocessed meat), it is impossible to disentangle the individual effects that each of these variables may have on risk.”

Interestingly, geographical distribution also differentially affects results, as positive associations are more commonly observed in United States populations and less commonly observed in European and Asian cohorts. The typical American consumes a portion of red meat alongside a bun made of heavily refined grain, a tall glass of beer or soda, and chips or fries cooked in industrially processed vegetable or seed oils, any of which could be responsible for the observed increase in cancer risk rather than red meat itself. Even when observational studies use statistical methods designed to adjust for these factors, residual confounding often remains. Bias may also play a role in influencing information found in the scientific literature, as researchers may be more likely to report positive associations than null associations.
Even if diets rich in red meat were conclusively shown to increase the risk of developing colon cancer, consumption of resistant starch in the form of high-amylose maize starch (HAMS) may counteract any pro-inflammatory metabolites formed by the fermentation of red meat in the colon. Adding resistant starch to a diet high in red meat causes colonic fermentation to switch from protein substrates to carbohydrate substrates, the latter of which can result in SCFA production. Inclusion of resistant starch in the context of a high-meat diet may therefore confer protection against the formation of DNA-damaging adducts.
Does organic matter?
In 2015, the International Agency for Research on Cancer classified three organophosphate pesticides used in agriculture (the herbicide glyphosate, the active ingredient in Roundup, and the insecticides malathion and diazinon) as probable human carcinogens (group 2A) based on occupational exposure studies in humans and laboratory studies in animals.
A 2018 observational study published in JAMA Internal Medicine followed nearly 69,000 French adults (78% were female with an average age of 44 years at the beginning of the study) over a four-year period and concluded that individuals consuming primarily organic foods were 73% less likely to develop non-Hodgkin lymphoma and 21% less likely to develop postmenopausal breast cancer compared to those who seldom ate organic foods, a result that the authors attribute to lower exposure to pesticide residues.
However, these results should be interpreted with caution, as the study relied on self-reported food intake data and did not account for confounding health behavior biases. People may not eat organic foods for a number of reasons, such as cost barriers, limited availability, or lack of interest, but the authors treated all nonconsumers equally in their analysis. Individuals who choose not to eat organic foods despite having the means may be indifferent to their health status in general, which would affect the findings.

Dr. Jorge E. Chavarro, an associate professor in the Department of Nutrition at Harvard T.H. Chan School of Health, co-authored an invited commentary on the study in which he described another study limitation: “The authors imply that higher self-reported intake of organic foods serves as a proxy measure for lower exposure to pesticide residues from food. However, they offer no empirical evidence that this is the case.” Nonetheless, the assumption is supported by previous research that demonstrates consistency between self-reported dietary intake data and urinary levels of organophosphate pesticide metabolites. Furthermore, the study does not account for varying levels of pesticide contamination in different types of produce, as eating some types of organic produce may offer more protection from pesticide exposure than others. Despite these shortcomings, the study provides justification for future studies to further investigate the relationship between organic food consumption and cancer risk.
Like what you’re reading? Follow Medical Myths and Models on Medium and sign up for our mailing list to stay connected!





