
The Cardiology Procedure That Revolutionized the Way We Treat Heart Attacks
The tandem discovery and perfection of angioplasty and coronary stent placement fundamentally transformed how heart attacks are treated.
I don’t recall the patient’s name, but I do remember his face. It was a face I had seen many times before. A middle-aged male contorted with chest pain. Morphine helped, but he was still in agony.
He was swiftly moved from the emergency room after an acute myocardial infarction (heart attack) was diagnosed to the cardiac catheterization laboratory.
One of my partners injected dye or contrast into his arteries and saw that one of his three main arteries was blocked entirely. This doctor inserted a thin metal stent, mounted on a soon-to-be inflatable balloon, to open the artery and restore blood flow within minutes. The patient’s pain was gone in an instant.
I practiced cardiology for 36 years, 1979–2015. Before 1986, we had no real treatment for a heart attack. Patients who had suffered a myocardial infarction (MI) were placed in beds for weeks and given pain medicines. We treated complications only. All we, the patients, and their families could do was pray they survived and not become a “cardiac cripple.”
Chemicals to Dissolve Blood Clots
Long before angioplasty and stents were used in blocked heart arteries, chemicals were used to dissolve blood clots thought to cause most heart attacks. Partial blockages of these arteries, like 75–99%, cause heart pains known as angina.
But when the blood flow gets sluggish enough, a blood clot forms, and then a heart attack ensues. Doctors speculated that injecting a blood-clot-dissolving chemical into a patient’s veins could restore normal blood flow. One such medicine was streptokinase.
It was first used to “stop a heart attack in its tracks” in 1958. However, its widespread usage did not occur until the 1980s. The advantages were that it did not require a cardiac or heart cath lab for administration. It was given via a peripheral arm vein. It worked 75–90% of the time. However, there were two problems.
One, the body has good and bad clots. If you cut your finger, the body forms a blood clot to stop the bleeding. That is a good clot. A blood clot in a heart artery causing a heart attack is bad. However, streptokinase cannot distinguish between the two; therefore, bleeding complications did occur with its use.
Patients with healing stomach ulcers covered by a clot bled. Other patients with previously undiagnosed brain artery aneurysms bled and often died. The second problem was that if the streptokinase was successful, it did not address the underlying problem, partially blocked arteries. And some arteries quickly re-blocked in weeks or months.
Genentech developed a safer but more expensive chemical, TPA (tissue plasminogen activator). Although bleeding was slightly less, it did not address the second problem. Because it is inexpensive and may be easily and quickly administered, streptokinase is still used in some poorer third-world nations.
The Game Changes
Everything changed thanks to the ingenious work of a German radiologist and cardiologist, Andreas Grüntzig. I never met the man at a course he started. I would take it in Atlanta, Georgia, in the late 1980s.
However, I did see many videos of him teaching and performing the procedure. He was tall and handsome with a black mustache. His lecturing style made you sit up and hang on to every word and sentence with only the slightest of accents.
Although he attended medical school in Germany, he eventually moved to Switzerland, where his pioneering work would start and blossom. Grüntzig advanced the work of an American radiologist, Charles Dotter.
In the mid-1960s, Dotter developed balloon angioplasty and later metal stents. He unblocked leg arteries, cured gangrene in a limb, and thereby eliminated the need for amputation.
In 1975, Dr. Grüntzig was the first to use angioplasty on a partially blocked human coronary artery in Zurich, Switzerland. He later relocated to Emory University in Atlanta, Georgia, where he was given better funding.
But Grüntzig took the novel approach to a blocked artery further, opening a 100% blocked coronary, or heart, artery that caused a heart attack. Angina, or coronary heart pains, were known to be due to less than total blockages of the coronary arteries.
Although medications helped, they did not cure angina. Complete blockages of these important heart arteries (there are usually three or four) usually lead to a heart attack if they happen suddenly.
He initially opened the partially blocked arteries by inflating a balloon strapped onto a thin wire and catheter that were threaded through an artery in the groin back to the patient’s heart while watching an X-ray.
The procedure was nicknamed an “angioplasty,” but the true moniker was a “percutaneous transluminal coronary angioplasty, " or PTCA. It was highly successful. However, many patients' blockages would reoccur over a few months and need another procedure. This complication was called “restenosis.”
The Birth of Coronary Artery Stenting
Dr. Grüntzig did not perform the first coronary artery stent procedure. Jacques Puel implanted the first coronary stent into a patient in Toulouse, France, on March 28, 1986.
Dr. Grüntzig improved and popularized the procedure. He postulated that leaving a permanent device, or scaffolding, inside the artery would be a more permanent solution.
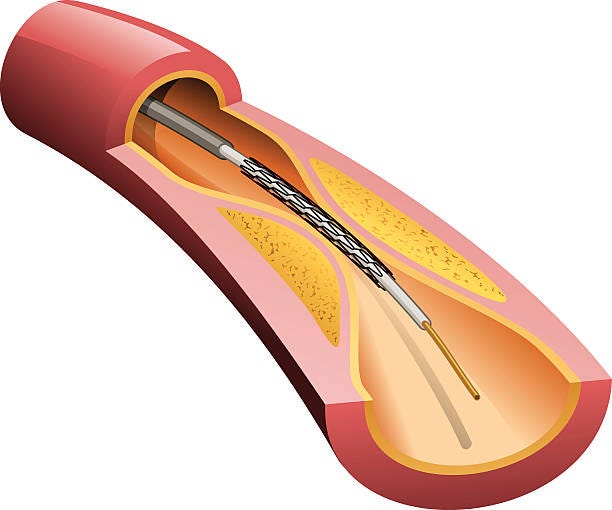
He mounted a deflated fine wire mesh jacket or stent (as shown in the diagram at the top) and then had the ballon inside it hold the stent open under pressure for several minutes.
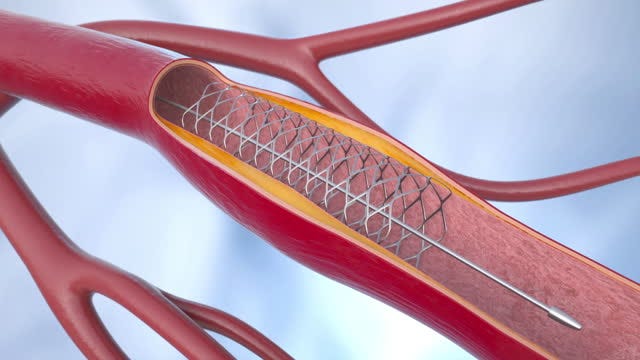
Next, he deflated the balloon, and the expanded stent would stay embedded in the artery wall, keeping the blood moving and the vessel open, as shown below. The procedure worked. The age of coronary artery stenting was born.
One of Grüntzig’s disciples, Geffeory Hartzler, was even bolder. In 1980, he used the procedure for the first time to abruptly stop a heart attack. The patient had immediate relief. This review of the history of PTCA and stenting is informative for those who want to learn more.
Sadly, in 1985, Dr. Grüntzig died while piloting a twin-engine plane during a Georgia thunderstorm. His wife of many years, Margaret Anne, died with him. Both are buried in Macon, Georgia. The Grüntzig Ethica Award for contributions to interventional cardiology is named for him.
Dr. Hartzler and many of Dr. Grüntzig’s other students continued to refine and improve the procedure. It offered a less costly, less painful, and more effective treatment for blocked heart arteries than open-heart surgery.
Dr. Hartlzler, known for his brash and self-confident persona, was heard to say more than once, “The only indication for bypass surgery is a failed angioplasty.”
For the first time, heart attacks could now not only be treated but rather cured.
Current State of the Art
“Each minute after a heart attack, more heart tissue is damaged or dies. Urgent treatment is needed to fix blood flow and restore oxygen levels.”
Oxygen, aspirin, and beta-blocker medicines have been shown to help. Yet, ultimately, the best course of action is to open the artery. Optimally, this should be done in the cath lab with coronary stenting.
Stents have been shown to reblock, or restenosis, with time. However, adding medicine inside the stents (drug-eluting stents) has decreased this late complication.
EMS and emergency rooms are keenly aware of this time factor. In a well-run system, there is no reason a patient should not be able to have his procedure in less than one hour.
The saying “time is muscle” is accurate and relevant. The time it takes for the heart attack patient to enter the ER door and start the procedure is known as " door-to-needle” time.
Ninety minutes is the maximum time for the best outcome of stenting a blocked artery after a heart attack. Indeed, many hospitals are rated by this time, which assesses the quality of their heart care.
However, it is incumbent upon the patient to recognize the signs of the heart attack and get to the ER as soon as possible.
Takeaways
- The treatment of heart attacks has evolved over the last 40 years. Powerful clot-busting medicines and physically opening blocked heart arteries have lowered the death rate and complications of heart attack victims. Better quality of life is another benefit.
- The science of physically unblocking arteries immediately has improved. It is currently the state of the art treatment, provided the patient enters the emergency medical system quickly.
- For the first time, it became possible to cure, rather than only treat, a heart attack.
- Some “old-fashioned” medicines, such as aspirin and beta-blockers, still play a pivotal and essential role in treating heart attacks.
- Poorer developing countries still use streptokinase for heart attack patients.
- A sense of urgency has developed in the modern treatment of heart attacks. Time = muscle has been the motto in this regard.
- However, it is incumbent upon the patient to get to the hospital as quickly as possible.
No matter how sophisticated the ER and hospital are, they still cannot treat a patient who is not there.
In this story, I provided a historical perspective from a cardiologist’s standpoint as a context for cardiovascular issues. My next stories will focus on practical ways to improve heart health and lower the risks of relevant conditions. I am a retired MD passionate about culture, health, sports, and food. Here’s some info about my background.
Thank you for reading my story. I wish you a healthy life.





