
The Art of Living With Persistent Pain
Never a simple prospect, in no small part because it seems like a ‘Groundhog Day’ situation from which there’s no escape, but with the right mindset and the right support, life can still be rich and fulfilling.
“When you arise in the morning, think of what a precious privilege it is to be alive — to breathe, to think, to enjoy, to love.” — Marcus Aurelius
I woke up this morning. I suppose I should be grateful for that — there are plenty ‘Think Positive’/’Choose Gratitude’ advocates out there who would tell me so anyway. The difficulty I had with cultivating an immediate sense of joyful sunshine was that I had a wall of pain in the way. As I have every morning, to a greater or lesser degree.
Every day I wake and lying still as possible mentally perform a body scan to assess where and to what degree pain is manifesting; whether or not it’s over and above a level at which I will be able to function fully; thinking about what I need to do that day and if there are any appointments booked, which may need to be cancelled depending upon how we (my partner and I) are feeling; whether I should take my ‘standard’ amount of tablets, or my ‘extra’ dose.
After coming to a rudimentary assessment, I usually attempt to limp to the bathroom and back. Mainly because my bladder is the size of a pea, also because it helps to see if I need to amend my thoughts on medication — and I can see if my twenty year old child is around to get the dog out and (preferably first!) bring me a hot cup of tea.
Actually getting out of bed takes variable lengths of time (and if I’m honest, often varying levels of swearing/cursing too). This morning, I got myself sat on the edge of the bed and sat in tears for a minute or two before hauling myself upright — beds with old fashioned frames and bed knobs are a friend to the ‘differently abled’ — and hobbling the few feet from one room to the next. It’s been getting worse recently and a return over the last couple of days to cold, wet weather has not helped me at all. I was in luck though, A (twenty year old) was awake and present, so was dispatched with the dog and a plea for tea.
Returning to bed a few minutes after I left it, I got back in and arranged a heat pad across my pelvis, switched onto a high setting to ease that particular area’s issue. I put on my gloves/wrist warmers and set my hands across the heat pad for a few minutes while I did the physio prescribed exercises for my neck and shoulders, then followed with my hand and wrist movements before putting my hands back against the heat pad. Once the pain had settled to a loud throb again, it was time to attempt to pop an array of tablets from their foil packing. This was accomplished fairly quickly today (just last night I catapulted one across the bedroom) and I took my morning medication then settled back with my phone on my lap to wait for it to begin to work.
My lovely hot cup of tea arrived and was set beside the bed. I was kissed on the forehead and asked if I wanted some breakfast too — but I wasn’t up for food yet, much as I appreciated the offer. I had an hour, reading a few articles online while sipping tea; rotating, crunching and flexing various joints; and being visited by fluffy family members. Some days I drift back off to sleep for a little while, but that didn’t seem to be on the cards today. My second rising was easier (though still painful) and I began moving around the kitchen, feeding cats, making another pot of tea, trying to get my body to co-operate before I needed to wake my partner.
You see, despite all of the physical problems I am living with, he is in a worse situation and I am officially his full time carer. Not that he doesn’t need full time care, but I am helped in this by A who has taken over much of the physical work (as well as a lot of housework and cooking), while I still look after all the ‘personal care’ needed.

As things stand today, during May 2022, I have been diagnosed with a number of conditions (see list below), which result in a combined and varying level of persistent (latterly ‘chronic’) pain and fatigue. As opposed to acute pain, which is sudden and sharp, but is relatively short-lived and tends to originate from an injury, chronic or persistent pain is defined as that which lasts longer than three months. As the first stirrings of my pain conditions began around forty years ago now, I think I can safely say that it does qualify as persistent.
I suffer with:
- endometriosis (and other gynaecological issues, including adhesions and ‘chocolate’ cysts)
- fibromyalgia
- osteoarthritis
- costochondritis
- post-viral myalgic encephalomyelitis
- hiatus hernia
- hypermobility
- neuralgia
- (I also have serious asthma, plus C-PTSD, clinical depression, general anxiety and panic attacks)
“My ‘good days’ are overshadowed by pain and fatigue, but at a level at which I can just about manage to keep moving through the day, look after my family of humans and animals, deal with any admin, appointments, etc and usually spare a little energy for my reading and writing. On my worst days, I still have to be sure everyone is fed, watered, and medicated correctly, at the very least — but these will also include a lot more pain meds for me, a great deal of being curled up with heat pads, soft blankets, clothes as loose as possible, naps, possibly tears and some help with my caring duties (for my disabled partner).” “I’m fine, thanks!”. But I’m really not ok | by Sadie Seroxcat | Being Known | Medium
I’m also ‘under investigation’ (yet again), because of ongoing irregularities with my blood panels, that have shown up consistently for the past twelve months. So there may be something else to add to the list at some point soon.

When it comes to treatment for my conditions, there have obviously been a variety of approaches, but mostly they have revolved around medication and nothing has worked particularly well. Strategies tend to focus on the elimination of pain, yet it is often the case that medication tends to merely blur the extent to which the pain is being experienced. Pain levels are not being dealt with, just masked — and there is an added problem when doctors cannot find a cause, a reason for your pain, and therefore choose to suggest that there is “nothing wrong with you” or that “it’s all in your head”, brushing off genuine pain problems as “imagined”.
Medical practitioners concerned with the physical have generally never been much good at seeing your body as a whole. They specialise or have an interest in their own area and that is all they see, there is no holistic view of what is going on in the rest of your body or thought given to how different conditions or symptoms might connect or interact with each other. Likewise, physicians have a tendency to isolate mental health as though your mind is not also a part of your body — and a very important one at that. So ‘all in your mind’, and other similar phrases, tend to be used dismissively…as though you genuinely are imagining your physical issues. Or worse yet, making things up, because you are ‘attention seeking’, or ‘drug seeking’.
A few years ago though, my local branch of the NHS (UK) introduced a new team, put together to work specifically with people who suffer from chronic pain conditions. They are known as the Persistent Physical Symptoms Service, or PPSS, and comprise of therapy oriented staff who have particular interests and training in chronic pain issues. There’s a physiotherapist, occupational therapist, counsellors who specialise in mindfulness, CBT, group therapy and the like, and also some highly qualified and trained psychotherapists with doctorates and specialist areas such as EMDR.
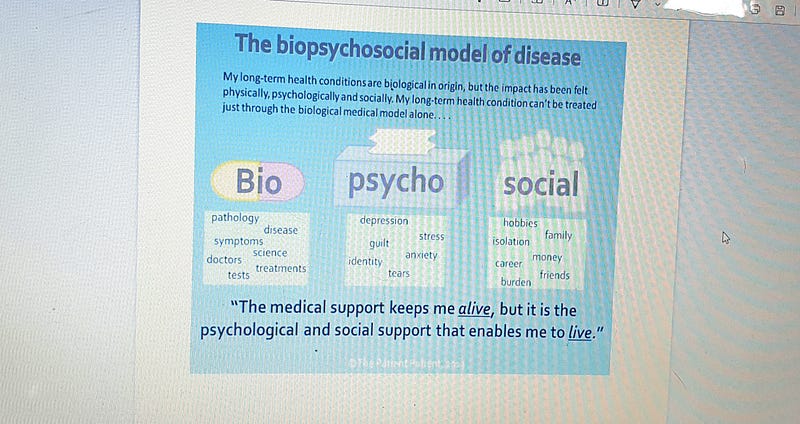
This PPSS team, who both my partner and myself have been referred to and worked with, have been an excellent resource, because they not only have their own specialist areas, but they work together and with a BioPsychoSocial model of healthcare.
What is the Biopsychosocial Model? - Proposed by Engel in 1977 - Views a patient as a complete person with a complex life - Behaviours, thoughts and feelings can influence the physical state - Includes the medical model factors alongside additional information THE-BIOPSYCHOSOCIAL-MODEL-OF-CARE.pdf (cumbria.nhs.uk)
Being able to see therapists who are part of the PPSS team has been helpful because it good to be able to talk to health professionals who are not inclined to meet you with disbelief and/or a quick brush off, coupled with a hastily dashed off prescription. Unless of course you have formerly been prescribed opioid analgesics to block your level of pain. I think we all know how difficult that situation has become in recent years (more so in the US, but it’s frowned upon in the UK too now, as a by-product).
Which also brings us to another issue commonly experienced when we are medicated for pain — side effects. Commonly experienced with opioid analgesics and other drugs prescribed for controlling and combating pain, are difficulties such as nausea, dizziness, drowsiness and mental confusion. Less commonly, seizures, stroke, cardiac issues, blood clots and more — not to mention the widely publicised potential for addiction. It’s also often really difficult (nigh on impossible), in my experience at least, to tell the difference between side effects from your meds and your original symptoms! But I digress…another piece may need to be written to go into the whole subject of prescription medication, this one already promises to be way longer than I can reasonably expect readers to deal with.
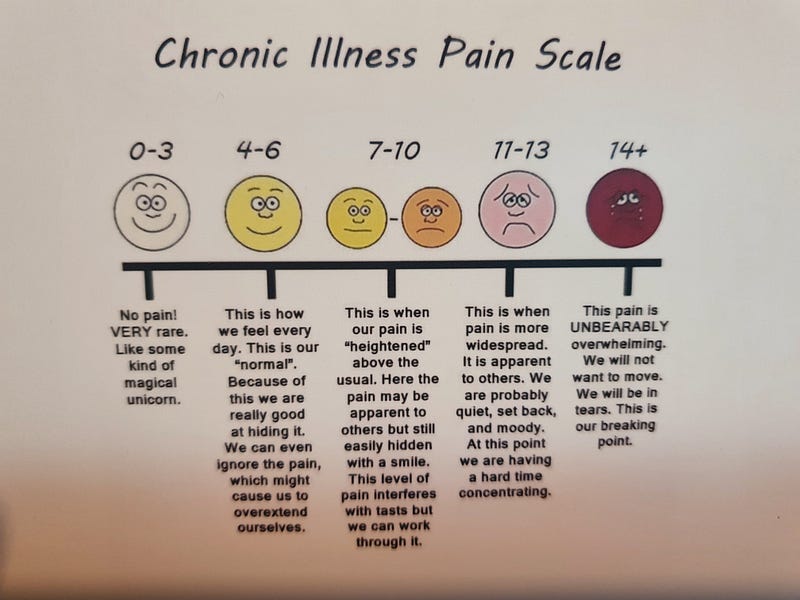
So on to the problem of pain scales. The first thing they ask you, whether you see a general practitioner (GP), a consultant/specialist or an emergency room nurse/doctor:
“Where is your level of pain on a scale of one to ten?”
It’s a ridiculous question. Pain is so subjective, the person experiencing it and the questioner will most likely not have anywhere near the same frame of reference, (though I suppose your answer might give them an idea of how close to your limit you are?) They say childbirth is one of the worst pains you can experience, but how does that help a male doctor understand anything? Or a woman who hasn’t given birth? Or someone whose birth experience was relatively fast and easy? And then there’s those like the gynaecology consultant who asked me to give him a number and then acted with incredulous disbelief when I told him. I mean, it’s a stupid question anyway, but definitely don’t bother asking me if you’re not going to believe my answer!
There are other pain scales in existence.
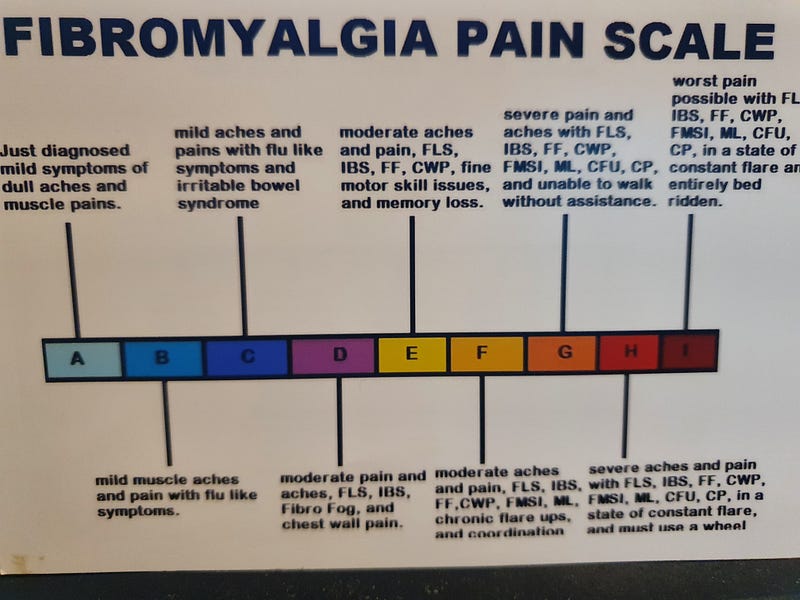
Though none are going to be perfect.
Personally I much prefer the Magill Pain Questionnaire:
The McGill Pain Questionnaire (MPQ) is a comprehensive multidimensional measure (Ahles, Blanchard, & Ruckdeschel, 1983; McGuire, 1995; Melzack & Wall, 1965; Wilkie & Monreal, 1999) that quantifies neurophysiological as well as psychological domains of pain. The MPQ, therefore, allows a comprehensive approach to measure cancer pain.
Reference: www.ncbi.nlm.nih.gov/pmc/articles/PMC3285427/
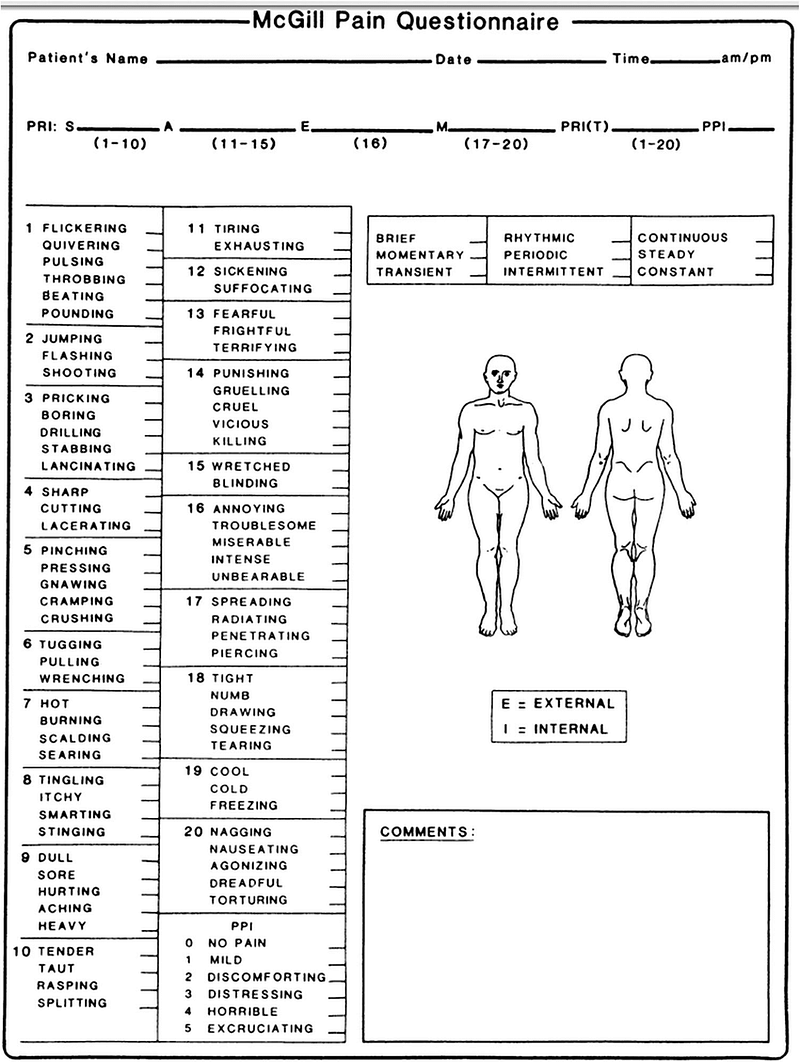
You can add a number for intensity if you wish, but only alongside an actual conversation which involves describing pain using actual descriptive words. At least try to understand exactly what a patient is experiencing. I understand that medical personnel are busy people, but it’s important to at least try to look like you care.
Which brings me back to the people I’ve been seeing who belong to our local PPSS team. They understand how important that show of care can be and they understand how living in a state of constant pain can wear on you. Can affect your mental health. They believe that looking after our mental health is just as important as physical care. I visited the team physiotherapist at one time, once a month for about six months. She saw to the much needed realigning of my neck and back, but during each session we also talked for a few minutes and I left feeling better for that too. She was a physical therapist, but because of the training she’d had as part of the team, she knew to check in on my mental health.
Similarly, the therapists whose main job is talking about Mindfulness or CBT will also check in about your physical health and discuss whether our needs are being met in that area.

In the case of the Psychotherapist who I see for fortnightly sessions, she in particular brings the whole biopsychosocial model into play. With her I discuss not only how I’m feeling (and why), we talk about all the different coping strategies I am using, the medication I’m taking and the ways I am coping on a day to day basis with both my physical and mental health challenges. The goal is to live my life as fully as possible, whilst accepting my limitations and working around them.
The two most useful therapies she draws from in our work are Acceptance and Commitment Therapy (ACT) and Eye Movement Desensitisation and Reprocessing (EMDR).
EMDR is beginning to help me process unpleasant memories and working towards eradicating my night terrors:
EMDR (Eye Movement Desensitization and Reprocessing) is a psychotherapy that enables people to heal from the symptoms and emotional distress that are the result of disturbing life experiences. Repeated studies show that by using EMDR therapy people can experience the benefits of psychotherapy that once took years to make a difference. It is widely assumed that severe emotional pain requires a long time to heal. EMDR therapy shows that the mind can in fact heal from psychological trauma much as the body recovers from physical trauma. When you cut your hand, your body works to close the wound. If a foreign object or repeated injury irritates the wound, it festers and causes pain. Once the block is removed, healing resumes. EMDR therapy demonstrates that a similar sequence of events occurs with mental processes. The brain’s information processing system naturally moves toward mental health. If the system is blocked or imbalanced by the impact of a disturbing event, the emotional wound festers and can cause intense suffering. Once the block is removed, healing resumes. Using the detailed protocols and procedures learned in EMDR therapy training sessions, clinicians help clients activate their natural healing processes. - What is EMDR? — EMDR Institute — EYE MOVEMENT DESENSITIZATION AND REPROCESSING THERAPY
ACT on the other hand helps me navigate daily life with chronic pain conditions.
If your efforts to control pain take up lots of energy and don’t work long term, ACT offers a radically different approach by helping you to let go of the struggle with pain and the constant pursuit of pain relief. This involves learning strategies to make space for the pain to be there, when doing so allows you to do things you want to do.
To better understand this approach, imagine you’re in a swimming pool and trying to hold an inflatable beachball under water, a metaphor I’ve adapted from the guide The Big Book of ACT Metaphors (2014) by Jill A Stoddard and Niloofar Afari. The beachball represents the pain — and thoughts and feelings about the pain — that you’ve been trying to control or avoid. You may be able to push this beachball under water for a while and this makes the pool appear calm. However, your arms soon get tired, and the ball eventually shoots back up. While you’re holding it down, the ball also stays very close to you. Holding down the ball makes it difficult for you to swim and splash around and have fun.
ACT helps you learn how to let go of the ball so that it rises to the surface of the water and floats around. This gives you the freedom to choose what you want to do in the pool and have more fun — maybe some gentle laps or even a big old canon ball! - How to live well with persistent pain | Psyche Guides
There’s temptation to fall into the trap of trying to use ACT as nothing more than a way of just relearning how to push aside our needs and gritting our teeth against the pain return to work. Some doctors take on the task of rehabilitation for chronic pain patients as though the goal is merely to get us back into work. However, work is not all there is to life. Some of us are lucky enough to have jobs which fulfil needs other than providing money to live on, but for most of us, we need to look elsewhere for the things which make our lives worth living. Therefore framing the most important aim of pain management as being to ‘get back to work’ is a mistake. Whatever it is for us that makes life fulfilling and worth living - the things we are interested in, passionate about - those are the things we most value and therefore the things which will help us to keep going when faced with day after day of pain and difficulty.
“The goal of ACT is to create a rich and meaningful life, while accepting the pain that inevitably goes with it. ‘ACT’ is a good abbreviation, because this therapy is about taking effective action guided by our deepest values and in which we are fully present and engaged. It is only through mindful action that we can create a meaningful life. Of course, as we attempt to create such a life, we will encounter all sorts of barriers, in the form of unpleasant and unwanted ‘private experiences’ (thoughts, images, feelings, sensations, urges, and memories). ACT teaches mindfulness skills as an effective way to handle these private experiences.” - Dr. Russell Harris, ‘Embracing Your Demons: an Overview of Acceptance and Commitment Therapy’, Psychotherapy in Australia, Vol 12 No 4, August 2006

“Try to learn to breathe deeply, really to taste food when you eat, and when you sleep, really sleep. Try as much as possible to be wholly alive with all your might, and when you laugh, laugh like hell. And when you get angry, get good and angry. Try to be alive. You will be dead soon enough.” - Ernest Hemingway
I am in pain all the time. Some days I can’t bear to do much more than curl up with heat pads and whimper. Other days though, I feel more alive — and I make the most of what I have and what I can manage despite the pain I’m feeling. I live my best life, under the circumstances, with my family and animals; my books and writing; and the beauty of the natural world around me. I may be seriously limited by my health, but I know what I value, I know my priorities and I love what I spend my days doing. I’m content and I’m fulfilled.