Extracting Premolar Teeth for Orthodontic Treatment: The Risks
Patients Report Health and Aesthetic Consequences
Reviewed by Dr. Noel Stimson, Dr. Ben Miraglia and Dr. Skip Truitt
Graphics by Alexandre Ruze
Today when a patient goes to get orthodontic treatment, there is a chance that the orthodontist will say that adult teeth have to be extracted: usually 2 upper premolars and/or 2 lower premolars (and perhaps 4 wisdom teeth). The patient might be concerned: is it a good idea to extract healthy adult teeth? Are there any consequences to losing these teeth?
Searching the Internet for answers, they may find claims that extracting premolar teeth can lead to “flattened” profiles and recessed jaws, and assertions that these are just rumors. They may see posts on social media of patients grateful for their beautiful new smile as well as posts from patients complaining Extractions have ruined my face! They might also come across reports that orthodontic extractions can lead to longterm serious health issues such as temporomandibular disorder, jaw joint damage, chronic neck/shoulder pain, a reduced oral cavity, tongue space constraint, narrowed airways and breathing disorders such as obstructive sleep apnea.

Do these negative reports have any basis in fact?
Before turning to an orthodontist for a response, people should be aware that the orthodontic specialty is also troubled by this question and has been for a long time. Orthodontists have been debating amongst themselves whether Premolar Extraction/Retraction (PER) damages the face for the past eight decades, ever since American orthodontist Dr. Charles Tweed first promoted the controversial PER method at an orthodontics conference in 1940. This debate is ongoing and unresolved today, and is so charged that premolar extraction is termed in-house the “greatest controversy in orthodontics.”
The public is for the most part unaware of this in-house “great controversy,” one that divides orthodontists into two opposing camps: one camp arguing that PER is a benign and excellent way to approach treatment, the other that it is a damaging method to be avoided in all but rare cases. Evidence is produced for both sides.
Which side is right? To hone in on the answer, this article first gives the inside details of this ongoing in-house controversy and then turns to the input and testimonies of patients (with photos). This will be the first time that the history of this controversy, well known within the profession, is vulgarized for the public. It is also the first time that the perspective(s) of the orthodontic specialty and the experience of actual patients are counterpointed.
A Quick History of “The Great Controversy” of Orthodontics
What is behind this controversy is the fact that in the early days of modern orthodontics, orthodontists did all their cases with no extractions, even those with very crowded teeth. The founder of modern orthodontics, Dr. Edward Angle, had been adamant that all 32 teeth had to be kept for a healthy full smile. For the forty years that he led the profession (1890–1930), orthodontists followed his strict philosophy that extraction went against the aims of the specialty: beauty and function. Instead of extracting teeth so that crowded teeth could fit on small jaws, these early orthodontists expanded the jaws so all 32 teeth could fit. Indeed extracting healthy adult teeth was by Angle’s time considered a barbaric practice, last done in the nineteenth century by barbers in barber shops.
Hence when Angle’s favorite student, Dr. Charles Tweed declared that extraction was not only acceptable, but in his view the ideal way to approach an orthodontic case, his speech met with outrage and protest. How could Tweed go against his mentor and the principles of the profession? Tweed’s argument was that extracting teeth would be the best way to prevent relapse, i.e. teeth moving back to their original positions (which was and remains a major problem for orthodontists). He also argued that the reduced jaw line, smaller smiles and flatter lips that resulted from extraction/retraction were “more pleasing” than fuller faces and bigger smiles.
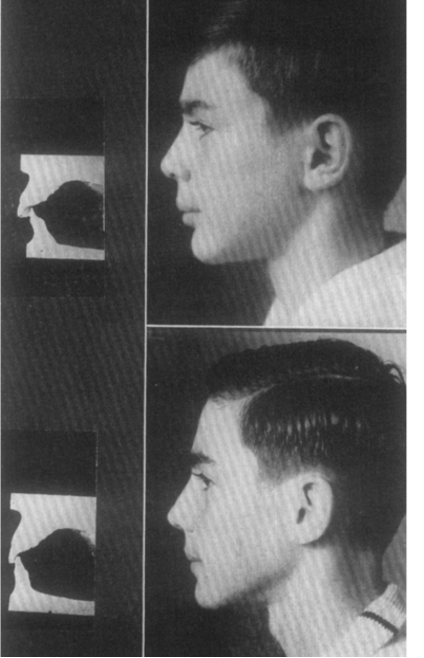
His colleagues countered that Tweed was wrong. Did this boy in Tweed’s case study truly look better with smaller jaws and a more retrusive smile? Couldn’t his changed neck curve post-treatment — i.e. his forward head posture — be an indication of unfavorable cranial changes? One of the most critical of Tweed’s extraction method and the unfavorable cranial changes it produced was the future President of the American Association of Orthodontics (AAO) and Chief Editor of the American Journal of Orthodontics (AJO-DO), the eminent B. F. Dewel. Over the course of the next decade, Dewel illustrated with dozens of case studies, in several erudite articles, how Premolar Extraction / Retraction holds back jaw growth in children and causes the mandible to fall back and downward.
Another renowned orthodontist, Dr. Alexandre Sved, went further and warned colleagues that if they were to jump on the bandwagon of extracting teeth, they would be ruining future generations of Americans by narrowing their smiles and flattening their faces. Yet another wrote — a decade after Tweed’s method had already come into use — that if orthodontists were to “go overboard with the 4 premolar extraction routine,” they would later be ashamed to run into their former patients and see their “caved-in” midface, like that of an edentulous person in advanced years who has “lost too many key teeth.”

Still the extraction practice took off and by the 1960s premolar extraction/retraction was being done in 70% of all orthodontic cases in the United States. Extraction was reputed, following Tweed, to cause less relapse (an idea that later proved to be wrong), and meant a faster treatment time than non-extraction treatment, hence cheaper costs.
By the 1970s premolar extraction/retraction had become a “standard of care” worldwide and an uncontested staple of orthodontics.
1970s: Premolar Extractions Linked with “A Flattened Face”
In the 1970s, alarming reports about the “flattened face” that resulted from extraction/retraction — nicknamed “the American orthodontic look” — drove the US extraction rate down to 50%. An OpEd was published in the New York Times, warning parents not to let orthodontists extract their children’s teeth. Renegade orthodontists published “twin studies” comparing one twin who had premolar extractions with the other twin who did not, showing notable differences.

These twin studies became the first scientific proof that the changes to the patient’s face after extraction orthodontics — such as receding chins and smaller mouths — were not just due to natural development.
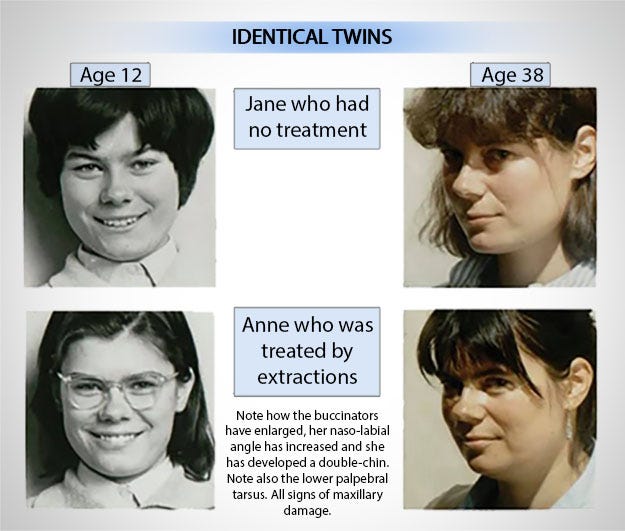
This first wave of scrutiny of the effects of orthodontic extraction focussed exclusively on the potential aesthetic changes, and notably did not address potential health consequences. This focus on aesthetics may have been due to the fact that most orthodontic treatment is for aesthetic aims, but it was also due to the fact that few orthodontists at that time were aware that there could be any health consequences. The orthodontist responsible for the fraternal twin case below, for example, felt terrible about what he had done to the extracted twin’s appearance with which this twin was deeply unsatisfied (and which led him to develop Damon expansive braces for non-extraction treatment), but he did not comment on the health risks that the flattening of her face signified. It was only in the next decades that research studies began to appear on the potential health consequences of extractions, correlating the “flattened face” with temporomandibular joint disorder (TMD), a reduced pharyngeal airway and other disorders.

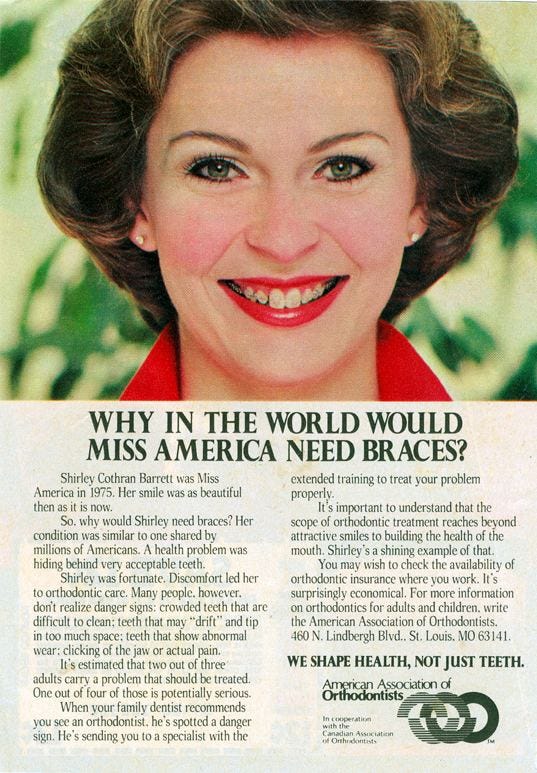
Impervious to these studies proving that PER causes facial changes, the official stance of the orthodontic specialty remained (and remains) that any facial changes reported after extraction orthodontics must be due to the way the child genetically was geared to grow and had nothing to do with the extractions. Beginning in the 1980s, a slew of research articles cropped up in orthodontic journals claiming that the “flat face” consequence was a myth. One key research study even determined that extraction/retraction only creates “excessively dished-in faces” in 10–15% of patients and hence was nothing to be concerned about. The American Association of Orthodontists (AAO), most concerned about how the stigma of flattened faces could damage the specialty’s reputation, launched an advertisement campaign to reassure the public that orthodontics does not always flatten faces. Miss America was recruited as the poster child for this campaign.
In what seems contradictory, at the same time that the orthodontic specialty made efforts to deny that extraction/retraction flattens faces, it also made efforts to lower the extraction rate to avoid the flattening of faces. The rate lowered from 70% in the 1970s to 50% of patients by the end of the 1980s.
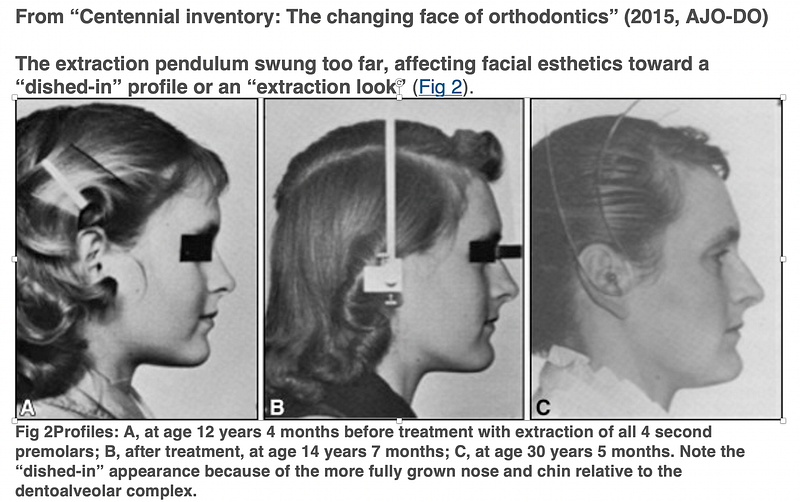
Today the American Association of Orthodontists (AAO) will still not acknowledge to the public the established fact that extraction/retraction can flatten faces. In-house, however, it does acknowledge it. In a historical overview of the first hundred years of American orthodontics, published in the AAO’s own trade journal (AJO-DO 2015), the section devoted to the 1970s explains that it was in this decade that the American orthodontic community became aware that they had “flattened” and “dished-in” the faces of “too many patients” with Premolar Extraction/Retraction, and in recognition of the significant facial damage (“the half-moon profiles”) extraction had caused, began to swing the “extraction pendulum towards non-extraction.”
The orthodontic specialty’s recognition that extractions can produce flattened and dished-in faces is in fact the reason according to this AAO centennial inventory that the premolar extraction rate declined.
Still, despite this published industry admission that “too many faces” have been “dished-in” and “flattened” by the practice of PER — and despite other research articles (like this one) that attribute the extraction rate decline to the unattractive “reduction of profile convexity” caused by PER— today orthodontist associations worldwide, including the AAO, will respond to patients who complain of facial deformity following PER that any “detrimental effect on a patient’s profile” (and any consequent health problems) must be due to “other causes” or “natural aging.” See as a case in point this 2021 email response from the British Orthodontic Society (BOS) to a 28 year old patient who complained of severely negative changes to her facial structure and to her health following her extraction/retraction orthodontic treatment. In their response, the BOS attributes the negative facial changes this 28 year old young woman witnessed after her extraction orthodontics (“deep folds around my mouth, flat mouth, retracted lower jaw, loss of upper lip”) as well as the health symptoms she developed (“jaw pain, clicking, grinding, locking, clenching, neck pain, migraines, ringing in the ears”) to “the normal aging process.”
To date, new patients are not disclosed that Premolar Extraction/Retraction orthodontics can flatten or dish-in their face, or make any changes to the face. If asked, orthodontists will normally tell patients it is a myth.

1986: Premolar Extractions Linked with Temporomandibular Joint Disorder: The Brimm vs Malloy Lawsuit
A new jolt to the orthodontic specialty came in 1986 when 19 year-old Susan Brimm sued her orthodontist for the severe jaw damage that resulted from her extraction/retraction treatment, and was awarded 1.3 million dollars for what the jury termed “deformation of her jaws” (Brimm vs. Malloy 1986). Following this verdict, the premolar extraction rate in the United States immediately dropped again, this time by half. If there was one Susan Brimm, there could be hundreds of thousands, and the growing specialty could not risk more million dollar lawsuits. Orthodontists began using palate expanders in children to avoid extractions, just like Angle did sixty years prior. Concern was also raised within the specialty that orthodontists had better take the temporomandibular joint into account when planning cases.
Paradoxically, however, at the same time that concern was raised in-house about the link between orthodontic treatment and the temporomandibular jaw joint, a concerted effort was made to disprove the validity of the Brimm verdict and the link it established between orthodontic treatment and the temporomandibular jaw joint. The American Association of Orthodontists paid for and commissioned a series of research studies that proved “with high quality evidence” that teeth had nothing to do with the jaw joint. Also reassuring the shaken profession that the Brimm verdict was nothing to worry about, an editorial in the AAO trade journal entitled “Tempest in a Tea Pot” (1992) advised colleagues not to panic about the fact that a “mere state court of law” had found PER to cause severe jaw joint damage. According to its author, who was both an orthodontist and a lawyer, why should orthodontists change the way they treat patients just because of a legal verdict? “A jury of laymen should not and does not set professional standards!”
The Brimm Case was in effect brushed under the rug. Today few orthodontists outside the United States have heard of it. The AJO-DO’s “centenniel inventory” of orthodontics does not even mention the Brimm Case. It notes that the extraction rate dropped dramatically in the 1990s and that “the temporomandibular joint” and “function” suddenly became a concern to the specialty, but it does not mention that the spur was the Brimm vs. Malloy verdict.
As for the public, it remains ignorant of this crisis in orthodontic history and the link established in a court of law between temporomandibular joint disorder and premolar extraction/retraction. There was no Internet at that time, and only a few newspapers covered the million dollar verdict, the largest award ever reported for dental malpractice.

Behind the scenes, however, the Brimm Case continues to have a powerful effect, spurring studies on the connection between orthodontics and TMD up until this day. For example, in 2015, a survey of 172 orthodontists in Brazil was launched to ask whether they believed orthodontic treatment can cause TMD: the question raised by the Brimm vs Malloy lawsuit. The result of this survey, disturbing to the survey authors who state that the articles commissioned after the Brimm Case had definitively answered this question, and the answer was no, was that the majority (52%) of the orthodontists believed yes, based on their empirical knowledge and experience, orthodontics can cause TMD. In 2018, to take another example, a study of South Korean adults established that orthodontic treatment could be related to increased symptoms of TMD. Then in 2022, a research study came out specifically on the correlation between premolar extractions and TMD. This latest study, published in a high impact peer-reviewed journal, established that orthodontic treatment with premolar extractions changed the way the mandible functioned in 25% of the extracted/retracted patients studied — which could, according to the authors, be a cause of temporomandibular disorder, and a reason to avoid extractions.
To date, patients are not disclosed the risk of temporomandibular disorder with premolar extractions.
The 2lst Century: Premolar Extractions Linked with A Narrowed Airway
In the 2lst century, research scientists, using the new tool of 3-D Cone Beam analysis, established that extraction/retraction narrows the patient’s pharyngeal airway and is potentially a cause of serious breathing problems such as Obstructive Sleep Apnea and UARS. This new finding caused yet another stir within the “teapot.”
The majority of orthodontists reacted by denying the validity of this finding or if accepting its validity, arguing that the size of the airway is not a factor in Obstructive Sleep Apnea, since “able-bodied” patients can potentially “compensate” for their reduced airway with “their airway muscles” (See AAO White Paper on Orthodontics and Obstructive Sleep Apnea, 2019). Others reacted by taking courses to learn about the airway. A new orthodontic discipline came into being called “airway-focused orthodontics.” Airway-focused orthodontists and dentists aim to avoid extraction and retraction and any orthodontic procedure that narrows the airway and prevents full breathing. Some of these airway focussed professionals have taken a public stand. See, for example, this dentist on his YouTube channel, and this myofunctional therapist on TIktok.
To date, patients are not disclosed that premolar extraction/retraction carries an established risk of reducing the airway.
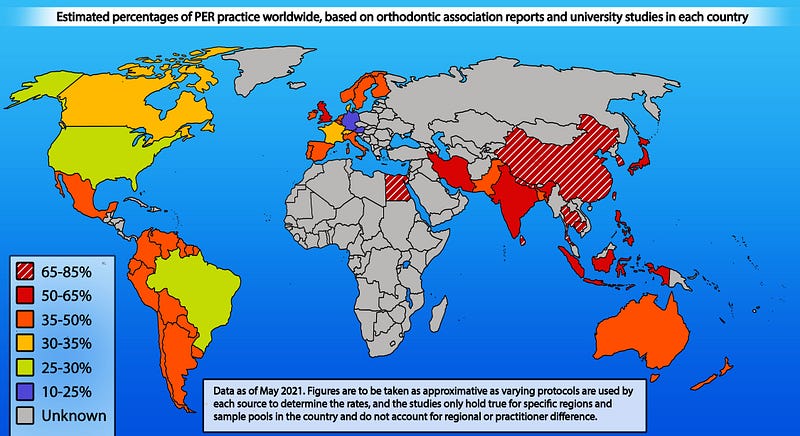
Rate of Extractions Today
Despite the steady drop in the extraction rate over the last century, the growing evidence of extraction consequences and the rising popularity of non-extraction orthodontics, today at least 1 in 4 American patients in orthodontic treatment get premolar teeth extracted. In most other countries of the world, the rate is much higher: from 50% to 87% of all cases, especially in Asia, Africa, the UK and Latin America.
In total, an estimated 7 million patients worldwide get healthy adult premolar teeth extracted for orthodontic treatment each year.
Are these patients — the majority of them children under the age of consent — at risk?
Risks to Health
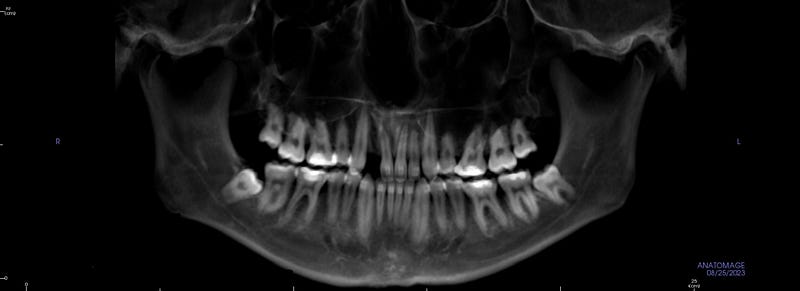
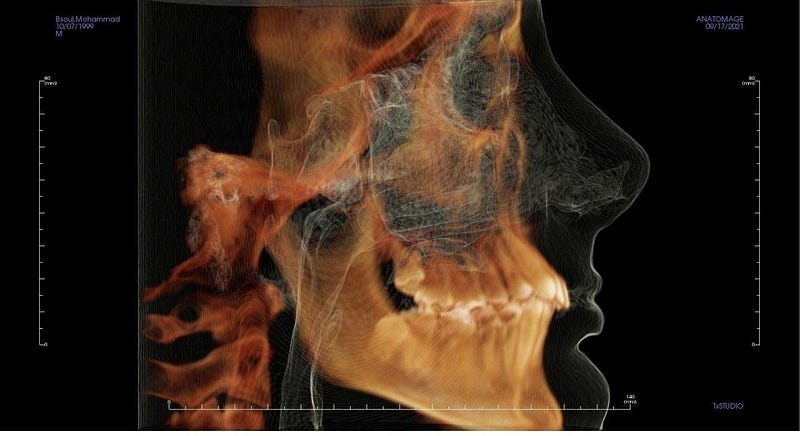
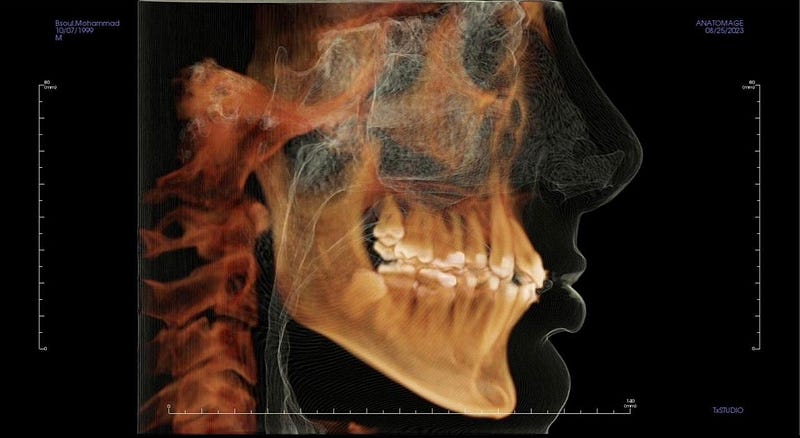
At the core of this question — and the 80 year “Great Controversy” — is the fact that extracting and retracting teeth does not just affect teeth. It makes permanent changes to the skull.
The changes to the skull include the following:
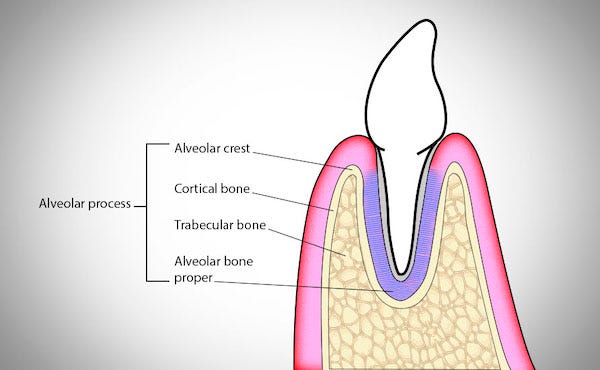
- Jaw bone loss. Along with the tooth, the patient loses the jaw bone that surrounds that tooth. The bone loss begins immediately with the extractions. It takes approximately six months for 60% of the bone in the alveolar process of the jaws — where the tooth was rooted — to decompose and resorb. The bone loss continues as the the extraction spaces “close” due to the orthodontic retractive forces (i.e. elastic bands or wires). This video shows how.
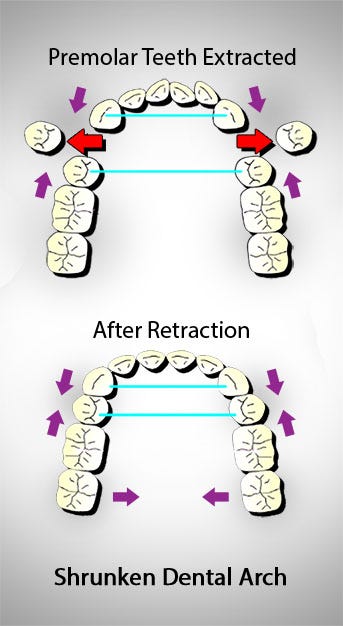
2. The alveolar ridge, which is a part of the jaw (its “process”), shrinks in size.

3. The dental arches shorten and narrow.
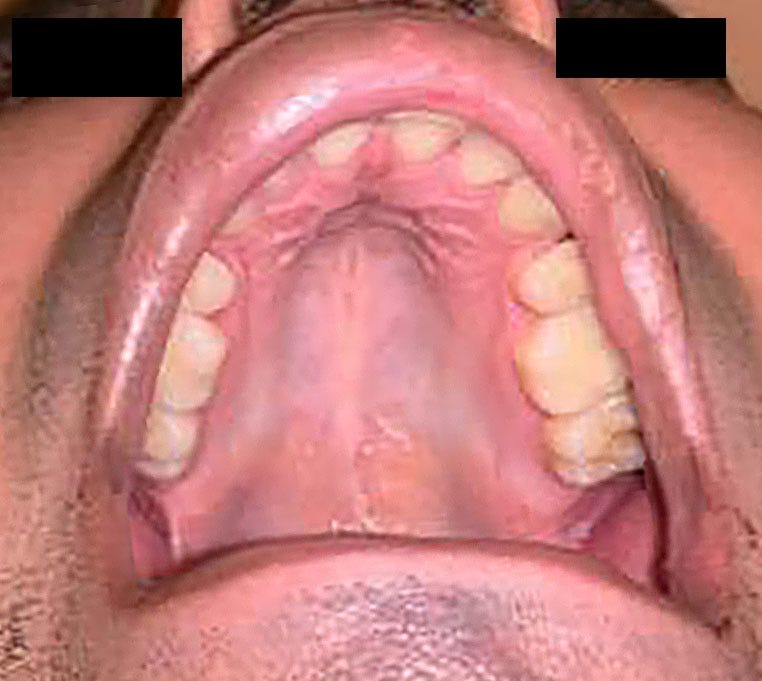
4. The palate — which is the base of the maxilla — shrinks.
5. The nasal passages — which is the same bone as the palate — shrink.
6. The oral cavity (mouth) becomes 1–3 cubic centimeters smaller.
7. The maxilla and mandible may grow back and downward in a patient who is still in growth.

8. The zygomatic arches (the cheekbones) may flatten.
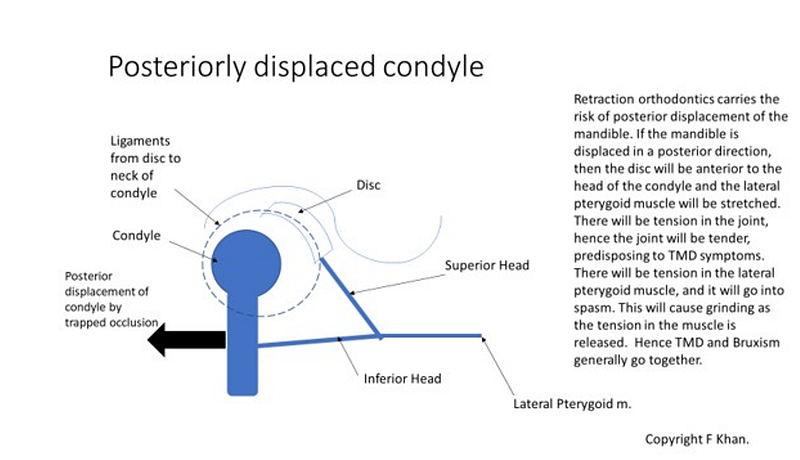
9. The condyles of the mandible may change position in the joint.
10. The hyoid bone may change position.
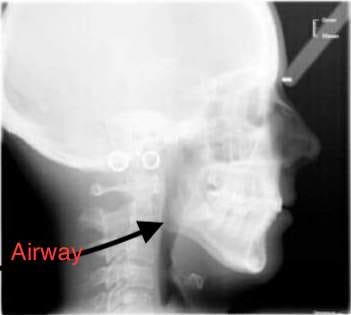
11. The pharyngeal airway will narrow.
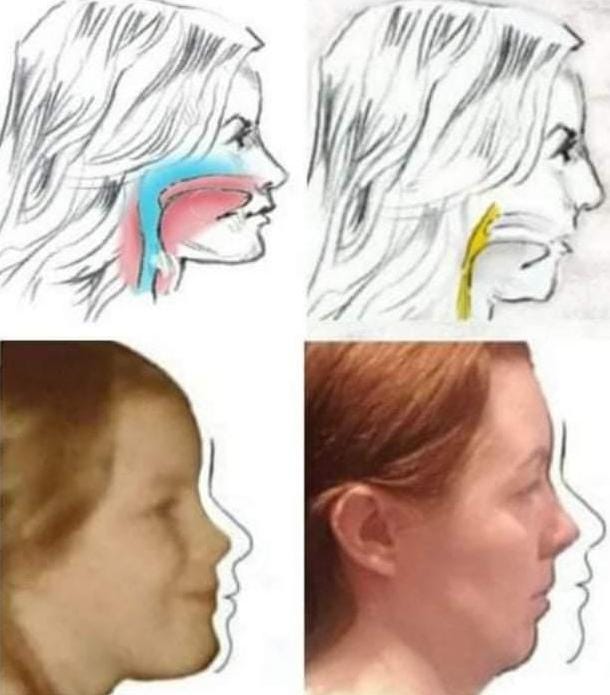
All the concern about the aesthetics of the “flattened face” masks, in fact, the real issue. It is not the face that is potentially flattened by premolar extraction/retraction. It is the skull. Changes on the outside of a face are signals of changes that have happened on the inside. A less full face means that the maxilla and zygomatic bones have insufficiently grown. A recessed chin means the mandible is retruded. A narrower smile means that the dental arches have narrowed and shrunk.
Each of these changes signifies or causes other internal changes. A retruded mandible means a smaller airway. Shrunken dental arches mean that the palate, nasal passages and alveolar ridge have shrunk.
A shrunken palate and shrunken alveolar ridge mean a smaller oral cavity (mouth).
A smaller mouth means a tongue with less space.
Less tongue space means that the tongue may be forced back towards the throat and may block and narrow the airway.
A narrower and/or blocked airway means less airflow. Less airflow means less breathing ability. This means that in waking hours, the patient may be forced to tilt their neck forward (Forward Head Posture) and lift their chin (Chin Lift) to open the airway and breathe.

A Domino Effect is produced. A retruded mandible, Forward Head Posture and Chin Lift will make the shoulders slump, the neck curve change and the lower back sway. Cervical vertebrae may compress. TMD/J may result from the retruded mandible. Somatic tinnitus may develop. Neck and back pain may develop. These issues may affect the nervous system.
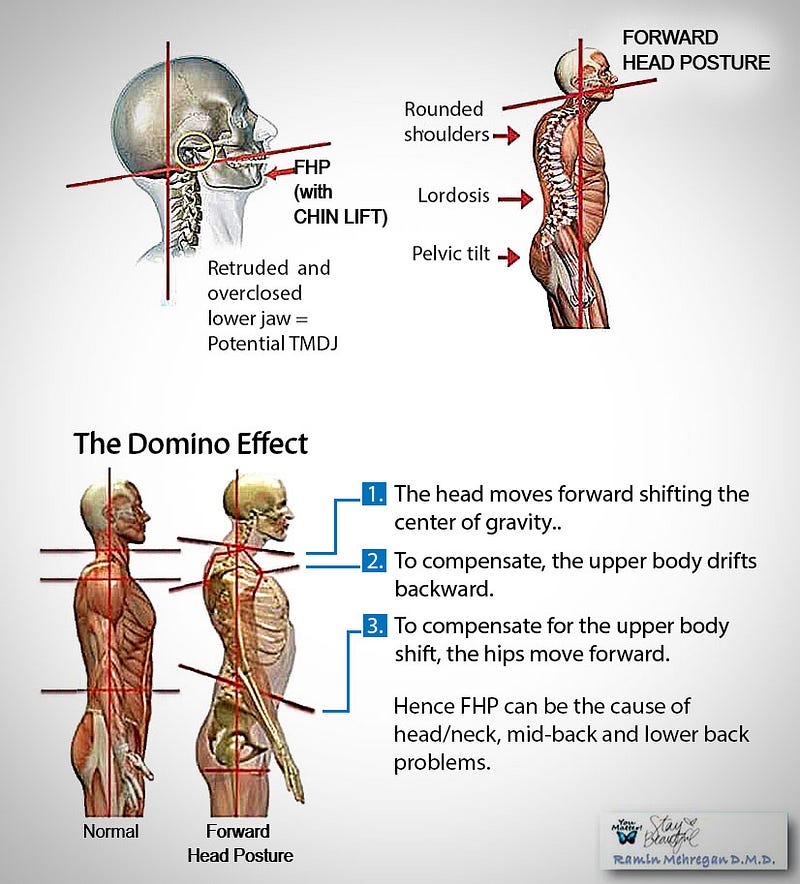
This is how the extraction of just a few teeth can potentially damage the entire body.
(For a detailed explanation of each of these points and a full bibliography of references, see the Report on Premolar Extraction/Extraction Consequences).
Yet the majority of orthodontists will tell patients, as they were taught in school, that there are no consequences to premolar extractions except a prettier smile.
What is the truth?
What percentage of extraction/retraction cases actually find themselves with recessed jaws, reduced dental arches, constricted palates, shrunken nasal passages, insufficient tongue space and narrowed airways, and how many develop chronic health issues later in life due to these changes: i.e. difficulty breathing, Obstructive Sleep Apnea (OSA), atypical deglutition, speech defects, bruxism, Temporomandibular Joint Disorder (TMDJ), tinnitus, Forward Head Posture, Chin Lift, cervical vertebrae compression, lordosis of the spine, inability to stand straight, and chronic neck/shoulder pain?
Nobody knows.
The only study published on the percentage of patients who get negative consequences from premolar extraction/retraction is the one that looked at how many get a flattened face and determined that “only” 1 in 7 PER patients at most are “excessively flattened” to the point of disfigurement. There have been no studies on how many extraction patients develop the same pattern of negative health consequences.
This omission raises serious questions given the by now five generations of patients who have undergone PER, the thousands of PER patients who have reported significant health problems (see Survey and Testimonies below) and the eighty years of heated in-house debate about the consequences of PER.
Two orthodontists who question this omission argue that there is indeed a crucial need for longitudinal studies of the health of extraction patients given that some of the health consequences of premolar extractions, such as OSA and TMD, tend to develop decades after the treatment when it is too late to trace an originary cause. Few are the adult patients who would suspect that their breathing difficulty, TMJ clicking or chronic neck pain could have anything to do with an orthodontic treatment done in childhood, and even fewer the doctors who could make such a diagnosis without precedent longitudinal studies establishing a potential link.
To date, however, no longitudinal health studies of PER patients exist. And none, the two orthodontists note, are likely ever to exist. Such studies would require considerable investment on the part of the orthodontic specialty, and, according to the authors, the orthodontic specialty is unlikely to want to make this investment.
To call a spade a spade, why would any established specialty want to find out if one of its bread-and-butter procedures causes severe health consequences in patients over the long term? It would logically be more in the specialty’s interest to find proof that these consequences do not exist. In fact, the majority of orthodontists’ articles published about health risks of orthodontic extractions (for example, the AAO commissioned White Paper on Sleep Apnea and Orthodontics, 2019 and the AAO commissioned articles post the Brimm Case) maintain the null hypothesis that there are no health consequences to extraction/retraction, and reveal a conspicuous lack of interest in scientific questioning of this null hypothesis.
A common design flaw exposes this lack of interest: the articles are all written by orthodontists and peer reviewed by fellow orthodontists. Orthodontists are not educated in the biology of the body (their focus in school is on teeth movement and mechanics) and hence lack the biological knowledge and competence to research the areas and functions of the body that extraction/retraction orthodontics can hypothetically affect: namely, the airway, tongue, jaws, hyoid bone and cervical spine, and deglutition, breathing, sleeping, jaw function, speech, proprioception, and posture. Sleep doctors, otolaryngologists, maxillo-facial surgeons, osteopaths, and myofunctional therapists specialized in these areas and functions of the body are rarely invited to participate in orthodontic studies of PER consequences.
As for the patients — the source of information — they have no voice at all. No former extraction patients have been surveyed or asked by orthodontists about their experience. There have been no follow-up longitudinal studies. Did they indeed get flat faces? Did their mandibles really retrude? Are their tongues squashed back? Did they like their new appearance after extraction orthodontics? Did they develop severe TMD or OSA later in life? Do they find it difficult to breathe? Do they snore? Did they develop postural problems, such as Forward Head Posture, scoliosis, cervical kyphosis, hyperlordosis or neck pain?
What percentage of patients regret having had premolar extractions? How many are happy with the result?
Aside from reports on the web from a patient here and there, a scattering of Internet patient forums on extraction consequences, and nine Facebook patient groups devoted to the topic of “reversing” Premolar Extraction/Retraction, there is no information on what actually happens to patients.
Patient Input
In an effort to rectify the lacuna of information about the patient experience, in November 2019, I launched an exploratory survey, distributed randomly on the Internet, to determine if and to what extent orthodontic treatment with the extraction of premolars correlates with adverse health and aesthetic issues. The first survey results with 114 respondents were published in Cranio UK (Winter 2020).
As of August 2021, 1299 patients representing 59 countries have responded to the survey.
Here are the results:
- 50.5% of the 1299 patients surveyed report 4 or more of the same health and aesthetic issues.
- 89% report that none of their health issues existed prior to orthodontic treatment.
- 29% report that a medical doctor has confirmed that their reported health issues were caused by Premolar Extraction/Retraction.
Health Issues Reported in Order of Frequency
- 61% report neck pain
- 57.7% report a feeling of inadequate space for their tongue
- 56.5% report Forward Head Posture (FHP)
- 56.5% report difficulty maintaining good posture
- 47% report TMD
- 40% report snoring
- 37.6% report TMJ clicking
- 35% report Obstructive Sleep Apnea
- 33% report tinnitus
- 30% report atypical deglutition (abnormal swallowing)
- 29.7% report speech or pronunciation difficulty
- 21% report UARS or other breathing problems
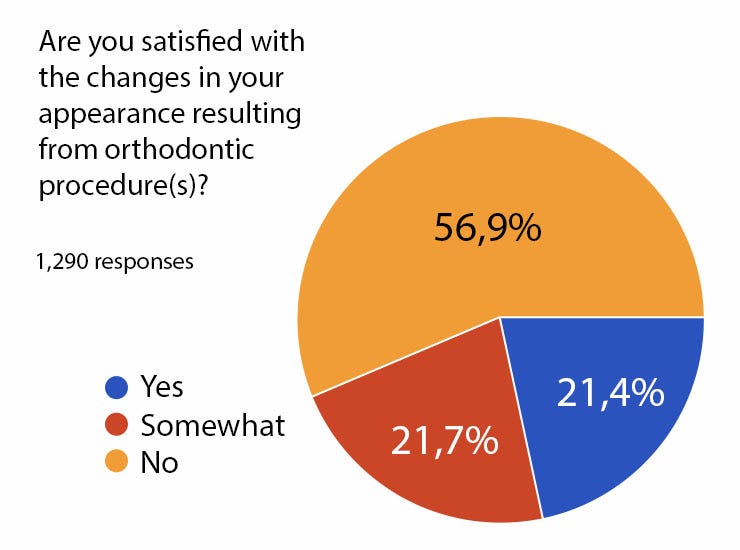
56.9% are unsatisfied with the changes to their appearance resulting from their orthodontic treatment.
Aesthetic changes reported in order of frequency:
- 65% report that their mandible retruded
- 48.2% report that their nose appears larger in relation to their mouth
- 47% report that their lips are thinner
- 42% report a prematurely aged appearance
- 37.7% report deep nasolabial folds
- 27% report dark circles or sagging under eyes
- 27% report a furrowed line in their chin
- 14.9% report a “bump” on the bridge of the nose, or a hooked nose.
In the section asking patients to comment on how PER had affected their life, 92% of the verbatims were negative. Comments ranged from “ruined it,” “destroyed it,” “made me permanently depressed,” “worst mistake of my life” to “not a day goes by when I do not think of all the suffering and pain this has caused me.” More than 35 of the respondents expressed suicidal ideation.
The survey the patients took is in this link.
To return to the question that spurred this article: does premolar extraction come with risks?
The answer appears to be yes. While the above percentages cannot be viewed as indicative of the actual percentage of patients negatively affected— as there was no control on the survey sample pool and hence a risk of self-selective bias (i.e. patients who were damaged are more likely to take the survey) — they establish that Premolar Extraction/Retraction can cause and has caused health and aesthetic damage in a number of patients.
838 patients reported the same pattern of adverse health and aesthetic consequences.
To put a human dimension to this number, I reached out to survey takers and asked if any would be willing to offer a testimony of their experience. Here are some of their testimonies below.
The overlap in their stories needs no comment.
Some of these testimonies have already been published in Cranio UK (Summer 2020).
Ballin B., 23, USA


Two years ago, my orthodontist removed two premolars on the top to make space for an implant for a lateral incisor I was missing my whole life. As the canines started moving back with rubber bands to “make space” for the lateral incisor, I noticed my front teeth moving back as well.
That is when my life quality started to decline. I now have a limit to how much I can speak. I get tired to move my lips and speak. My jaws are tired from trying to bite on my back molars to eat and to rest. It does not feel like they are in a natural position.
And my poor tongue, it is too big for my mouth now, with very little space to relax. I need help, and I need it fast.
I am looking for a new orthodontist to offer a solution ASAP, but I lack the resources to pay for a new treatment, so I hope my current orthodontist reimburses me.
Joe Morris, age 20, UK

My name is Joe Morris and I am a 20-year-old student studying economics at the University of Leeds. I had traditional ‘extraction-retraction’ orthodontics as a child. I started to notice that something was wrong as early as the first few weeks after my teeth were extracted.
But it was not until later in the treatment that I started to notice that something was really wrong. I noticed that my facial features were weak compared to my peers; my cheekbones were flat, eye support weak and my jaws had grown long and narrow.
My sleep became poor. I had excessive daytime sleepiness, poor concentration and fatigue, despite getting over 8 hours of sleep per night. Within weeks after the braces were removed, I developed severe TMD and muscular pain in my right temporalis. The pain was so severe that I was forced to seek assistance from an osteopath.
These afflictions started to markedly disrupt my high school life. Though I had a strong friendship group, I do not feel that I was able to truly ‘blossom’ like I would have without these medical burdens. Studying became exhausting. I was always in a sleepy haze. I struggled to stay awake in classes and focusing on problem-sets for long-stretches of time was arduous. Dealing with episodes of painful TMD made this even harder. Thankfully I was still able to achieve a high score (39/45) in my international baccalaureate program due to my stoicism.
At age 18 I began my degree at University. My weak facial features caused great insecurity, my sleep was now very poor and my episodes of TMD continued. I started to avoid socializing more and more and my grades started to plummet. By the first semester of my second year I’d reached my breaking point and I decided to seek medical assistance. Through my own research online and reading in academic journals I was able to determine that my afflictions stemmed from the unfavorable development of my jaws and face. Over the next few months I consulted with an ENT who diagnosed me with moderate obstructive sleep apnea syndrome (OSAS); a fairly heavy finding for an otherwise healthy 19-year-old. I was also able to consult with an alternative orthodontist who explained that the unfavorable structure of my jaws, and my ensuing TMD and OSA, had been caused by the inappropriate orthodontic treatment that I had received as a child.
Thankfully the University of Leeds was sympathetic to my situation and granted me a repeat of my second year of study and a year of temporary leave on medical grounds. In fact, they determined that given the severity of my afflictions, I would not be able to return until I provided proof that I was fit to study. During my year of temporary leave, I was able to consult with a number of other alternative orthodontists who were able to confirm that my afflictions were caused by the inappropriate orthodontic treatment that I received as a child. I started treatment with one of these alternative orthodontists in London. He is using a growth appliance to literally reverse the treatment that I had as a child. I have also started a trial of continuous positive airway pressure (CPAP) for my iatrogenic sleep apnea. I am currently in the process of deciding whether I will be fit enough to continue my studies before the beginning of the next academic year this September.
Rachel, age 44, London, UK

At age 9, my four first premolars were extracted for orthodontic retractive braces. I had blinding headaches and vomiting for months beginning at age 10. Then my shoulder, neck and general muscle pain started and, at age 12, my jaws started clicking. I had begun to play the violin at that time and my increasingly painful neck, shoulders and back was attributed to my playing.
As I had waited 5 years for the chance to have lessons, wild horses wouldn’t have dragged that violin from me and I shut up about the pain. I was told my clicking jaw was normal. Most children will try to accept anything if convinced it is ‘normal’; they have no experience with which to compare it. I was told the orthodontics were supposed to be painful and uncomfortable and so I accepted this.
My face changed rapidly. The skin on the bridge of my nose got so tight and shiny, I would have to powder it before school. It also began to seem bigger than my lower face, which had been retracted from the braces. I was so embarrassed. I would stand next to the double mirror in the bathroom daily, pulling my top lip and jaw forward to try to make my nose look smaller. The face grew down and backwards; my top lip practically disappeared.
I managed to struggle on, managing symptoms by going from pillar to post, massages, osteopaths and so on, until at about age 24, my body came to a grinding halt. I had had to abandon any thought of a career as a performing violinist. I was totally disabled.
The list of symptoms: daily blinding headaches, very severe neck pain, rigidity in my entire musculature, especially face and jaw muscles, numbness in my arms, post-nasal drip and constantly feeling shivery and fluey.
Over the next 10 years I went to 3 pain clinics, had every body part scanned, and tried every drug out there, nerve blocks, injections, psychologists etc. My jaw joints were finally scanned in 2005 and showed non-reducing disc displacement on both sides, condyles at the back of the joint, arthritis and bone loss. I have never been able to perform as a violinist.
Natalie, age 20, Adelaide, Australia
I was 12 when I underwent retractive orthodontic treatment, with all 4 first premolars removed, and concluded treatment at age 15. I have felt that something is off about my face ever since. My smile became gummier because my upper jaw and front teeth were pulled down with elastics, my face became longer and flatter, and my lower jaw became more setback due to the retraction and smaller size of my maxilla.
I developed a reverse swallow pattern during treatment, and started to develop TMJ issues due to the strain my unnatural lower jaw position puts on my joints. The results of the treatment have also taken a toll on my mental health and study: I read orthodontic case studies for hours on end in hopes of finding a ‘cure’ for what has been done.
Overall, I am deeply unsatisfied with the orthodontic treatment I received as a child. It has negatively affected my life, and will continue to do so, more than anyone (apart from those who have been affected by the same retractive treatment) could ever know. I have photos and x-rays depicting the changes in my face, and I feel so heartbroken whenever I look at them; when I look in the mirror, my face doesn’t feel like my own.
Emma Green, age 31, Dublin, Ireland
At the age of 14, the decision was made for me to get four premolar exactions prior to starting orthodontic treatment. I remember getting into my father’s car and crying my eyes out. It was my body’s natural reaction to getting four healthy teeth pulled. But the orthodontist told me I will have beautiful straight teeth if I got the extractions, so that gave me the courage to go through with it. I didn’t question it again, as I believed that the ortho must know more than me, he wouldn’t put my health at risk.
Flash forward: my teeth are now straight at a huge cost — my health and my aesthetics.
My palate was already small due to poor oral posture in early childhood. Now it is smaller and I can no longer fit my tongue on the roof of my mouth. It is quite suffocating and I feel claustrophobic in my own body. Due to the inability to rest my tongue on my palate my mouth falls open and I mouth breath. I find it difficult to exercise and run for a prolonged time. My airways are small. Since I finished my ortho treatment, I also suffer from TMD.
My teeth were pulled back into my face which is aesthetically unpleasing, and my maxilla was retracted which has resulted in my face becoming flat. My cheeks are sunken and my lips do not have sufficient support.
If I had known the implications, I would not have undergone this treatment. I would be better off if I still had crooked teeth and normal functionality. In an ideal world I would have tried to expand my palate to fit all my teeth in and avoid extractions. I am now in the process of trying to reverse my extractions by expanding the palate and reopening the spaces for implants. As an adult I feel that I need to take control of what happened to me and find a solution as I owe it to not only my past and current self but most importantly my future self.
Stefan, age 31, Sweden

I want to tell my story to make others understand that the model of removing and moving teeth to get a nicer smile is not always the best. In my case, my appearance and life were destroyed.
When I was 10 or 11 years old, I was diagnosed with crowded teeth. Nothing that affected my health, but due to how the Swedish healthcare system works, I was offered orthodontic treatment for free.
The treatment started when I was around 12. First, four healthy premolar teeth were removed, which neither I nor my parents had been informed about in advance. Metal brackets with wires were then attached to all my teeth in order to pull the teeth back to close the gaps created from the extractions.
Halfway into treatment I began complaining that my tongue was not fitting in my mouth and that breathing had become difficult. The treating team of orthodontists assured me that this was only a transitional phase, and that after a while my body would get used to it.

The treatment was extremely painful. I had daily headaches with severe pain in my mouth, jaws and face. I felt awful and was hugely affected by the pain with extremely poor sleep. In addition, I started to snore heavily while sleeping. I began to see stairs as huge obstacles. It was simply too difficult to breathe.
All this had negative effects on my grades and my schooling. I also could no longer attend school gymnastics or participate in leisure activities that involved any physical movement.
My appearance also started to deteriorate. My jaw line disappeared and my face flattened and recessed. At the time, I did not think these changes had anything to do with the orthodontics, but now in retrospect I understand that they were all due to it.
After several years of suffering, the braces were removed. I was now 17 years old. The treating orthodontists rated the treatment to be a success.
But for me it was a disaster. I sustained permanent damage from the braces. My health problems did not disappear once removed, as promised, but continued to worsen. The trachea had been compressed since my jaws had shrunk due to the retraction where the extracted teeth had been. A few years after the treatment, I had a new growth spurt where my body grew both in length and width, but my jaws remained reduced in size and my breathing further deteriorated.
Today I am 31 years old. The problems with lack of space for my tongue and difficulty breathing persist. My airways are narrow and my trachea is always under pressure since my jaws are too recessed, forcing my tongue and chin back into my throat. I snore, have sleeping problems and am forced to move around with bad posture to be able to breathe. I must lean my head forward and upward to get airflow, which causes chronic pain and tension in my neck and shoulders. I am constantly tired and have very poor energy. Consequently, I have never been able to work or pursue a higher education. I am being supported by the Swedish state.
I have spent all these years searching for solutions. I have visited about 30 dentists, almost as many orthodontists and most of Sweden’s maxillofacial surgeons. Not one of them could detect any bodily defects and I am therefore regarded as imaginatively ill and often treated badly by the care providers. Some of them have even said that my problems are all “in my head” and that I am mentally ill. None of them could even imagine, much less admit that any of my problems could have anything to do with the orthodontic treatment with extractions I had as a child. None have proposed tests on my breathing, my airway volume, or my tongue function.

The only recognition that I have received in Sweden on my orthodontically-caused health problems has come from an organization called Tandhälsoförbundet (tf.nu), a Swedish advocacy group working to make Sweden a better place for dental patients. One of their goals is to make the protective laws that exist for normal healthcare to be extended to dental care. They published this report on my case.
I continue looking for solutions. Two years ago, I had the hope of being treated by an orthotropic clinic in Norway where an orthodontist was going to try and restore my mouth as much as possible by expanding the arches forward. However, due to cost and treatment time I had to cancel those plans.
My hope has now changed to double jaw surgery, to achieve more tongue space and increase the airways. Surgery will give faster and more guaranteed results compared to the orthotropic route.There are risks involved but at this point I don’t care anymore; I just want to be able to breathe.
In Sweden though, one has to apply for eligibility for jaw surgery, and prove certain conditions, including, but not limited to, severe Obstructive Sleep Apnea. I have recently been accepted to be on the waiting list for a Sleep test. I am hoping to be able to finish all of the necessary tests before the end of this year, and that my OSA level will be severe enough to satisfy the Swedish requirements for eligibility for jaw surgery. Otherwise, I will need to go to another country and have the surgery there and pay for it myself, which will be difficult. Since I can’t work, my ability to finance the surgery is limited.
Update: Stefan’s spinal issues, caused by his narrowed airway, deteriorated to the point that he had to have his spine surgically fused in November 2023.
Max, age 30, New York
I’m a 30 year old male entrepreneur building a tech startup. My passion is music. At age 11, I had 4 bicuspid extractions. At age 25, I found out I had moderate sleep apnea, and severe Upper Respiratory Resistance Syndrome UARS (16.7 AHI, 32.7 RDI).
Since that diagnosis, it has been a bumpy road to find a treatment that works. I initially tried CPAP, then a prescription drug, modafinil, and next, a mandibular advancement device. Hopeless, I began doing a lot of my own research and came across airway focused orthodontics. Along the way, I met plenty of amazing health care practitioners who helped guide me; at the same time, I also met plenty who were not only not helpful, but even worse, told me my symptoms were all in my head.
I’m currently exploring options of reversal orthodontics with palate expansion, and for the first time in a long time, I feel hopeful. It is hard to fully express how debilitating this condition is. I struggle to work a full-time job, I had to move back in with my parents, and most frustratingly, I feel held back from fulfilling my dreams. It is a struggle just trying to get through my day. I’ve never really dated or been able to invest in building the types of friendships I want to because by the time work is done each day, I just want to go to sleep.
But now that I understand the underlying cause — my narrowed palate and retracted jaws-and how to go about fixing it, I’m confident one day I’ll look back at all these challenges and they’ll be a distant memory.
Nelly, age 38, Mexico City, Mexico
At age 34, I decided to get orthodontic treatment. The orthodontist extracted 2 premolars and retracted my teeth. Two years later, when the treatment ended, I began to experience great neck pain, and no space for my tongue in my mouth. I knew something was very wrong, and turned to at least a dozen orthodontists for help, including university professors of orthodontics at UNAM. Everyone said my orthodontic treatment was perfect. But I could not sleep. I was advised to see psychiatrists and told to take anti-depressants.

Nothing resolved my pain. I wanted to die, and thought if I do not kill myself, my own body will with my time. I convinced my orthodontist to move some of my teeth back out, and within a few months felt some strength come back. I did much research and tried to fight for my health, even though the people around me did not believe me. I asked other orthodontists to reverse the treatment completely, but nobody would take my case.
In desperation I tried to push my own teeth out with my hands, to give space for my tongue, and damaged the roots. I wrote to an orthodontist in California who offered reversal orthodontics, and another one in Italy. I could not afford the 300,000 pesos for treatment or the travel. I have not stopped looking for help, my symptoms are too strong, I can’t enjoy anything, and in the night I am awake and desperate with pain. I have turned to spirituality to help me.
Lydia Steiner, mother of a 15 year old, London, UK
I am the mother of a 15 year old UK musician and actor who was receiving serious international attention and had a very prominent career. Two years ago, he had premolar extractions and retraction with elastic bands. His health and face changed immediately for the worse. He woke at night gasping for air, and developed sleep apnea , terrible sinus problems, neck ache, jaw ache and back ache. More than that it has destroyed his confidence and possibly his career. His face has gone flat, both jaws have been forced back, his nose sticks out, he has lost eye support. My hope is that he can have his face partially back with double jaw surgery. He can no longer sing properly because the maxilla is responsible for depth and volume of voice. I cannot believe that retraction of a child s face is legal. It is barbaric and cruel.
Jose, father of a 23 year old, Chiappas, Mexico
My son had two premolars extracted and retractive orthodontics at age 17. His palate became very small and he has no space for his tongue. He has not been able to breathe well or sleep for the last four years. He is always awake. He cannot breathe through his nose. I am searching solutions for him now. Es una situación muy fea.
Update: Jose’s son has since had successful Lefort 1 surgery and IMDO mandibular surgery, by Dr. Antonio Piña in Puebla. His parents report that their son “now breathes.”
Nicole, age 45, Germany

When a teenager, I was a cheerful person, an optimist who approached people with self-confidence. I was a so-called sunshine who could make others laugh. I could express myself well and had a certain charm and was pretty. Once, a gym teacher asked me in front of others if I would like to model. Someone said that I couldn’t be a model with my slightly crooked teeth. I started to be ashamed of my crooked teeth.
When I was twenty-eight years old, I had two premolar extractions and braces.In the course of the treatment my facial fullness changed. I thought it was because I lost weight. I told the doctor. She could not explain it. At some point when the extraction gaps were closed, the dental arch in the upper jaw was so small that I could not get my jaw open properly. It seemed very tight and the canines were tilted too much inwards. Suddenly the front teeth were very steep and I noticed that I had problems with my jaw. It always clenched.

When I found out the extent of the damage to my jaw joints and my face, I broke down mentally. I started looking for solutions. Nobody could give me hope. The thought that that I was now forced to live permanently in pain and that my face would never look the way it used to, made me infinitely sad and angry. I felt powerless. I withdrew from all social contacts. I became very insecure. I lost friends because I isolated myself.
At that time I had been working for 1.5 years in a new company. I was supposed to build up a new area of customer care within the company and lead it with international contacts. The boss of the company had offered me this job because he knew me from a previous job and had experienced me as very tough and dedicated. But nothing was left of the once tough woman. I left my job and went home to live with my parents.
So far I have visited 12 orthodontists, 5 oral surgeons, 2 CMD specialists, 1 osteopath and 3 alternative practitioners, and have incurred costs of about 17,000 €. I now understand that the only way to regain the health of my joints and jaws is to reverse the orthodontic treatment. My upper jaw and lower jaw have to be moved forward somehow. I have not yet found a surgical procedure that gives me confidence.
In the meantime, I discovered forums where others reported similar experiences. We have met and gone to doctors together. We give each other strength and encourage each other. We exchange ideas about experts. I am also involved in educating people about the risks of extraction orthodontics. I have launched a survey to extraction orthodontic patients in Germany. I have written to associations in charge of orthodontics to complain about this problem on behalf of injured parties. They referred us to the Ministry of Health. Nobody contacted us again.
Through this experience with orthodontics I came across further problems in the health care system in exchange with people with medical problems in other areas. I recognized a social problem of recognition for all of us.
I must say that even though this treatment ended so disastrously for me, it has made me take a critical look at myself and our society. Today I am no longer the sunshine of life. I have become more thoughtful, more careful and more critical. I have opened my eyes to the less beautiful sides of life and I am glad that I have recognized, even if forced to, many things that I probably would not have otherwise. I am much richer in experience and knowledge.
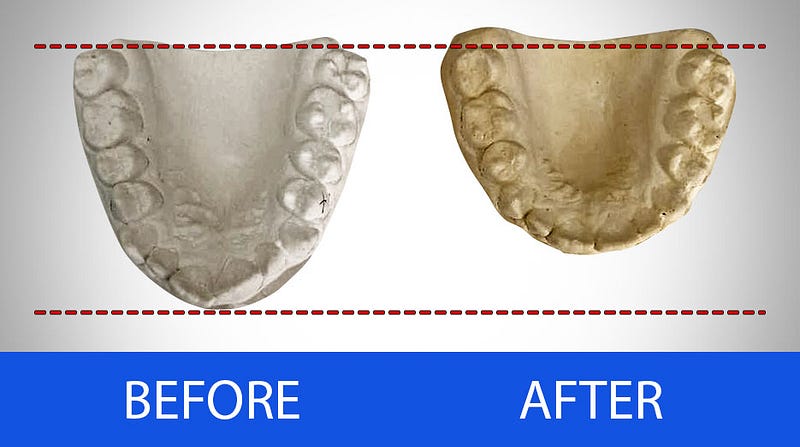
Nicole created a website (in German) on the risks of premolar extractions. Her case is featured on this website with xrays showing the changes to her occlusion and jaws from PER.
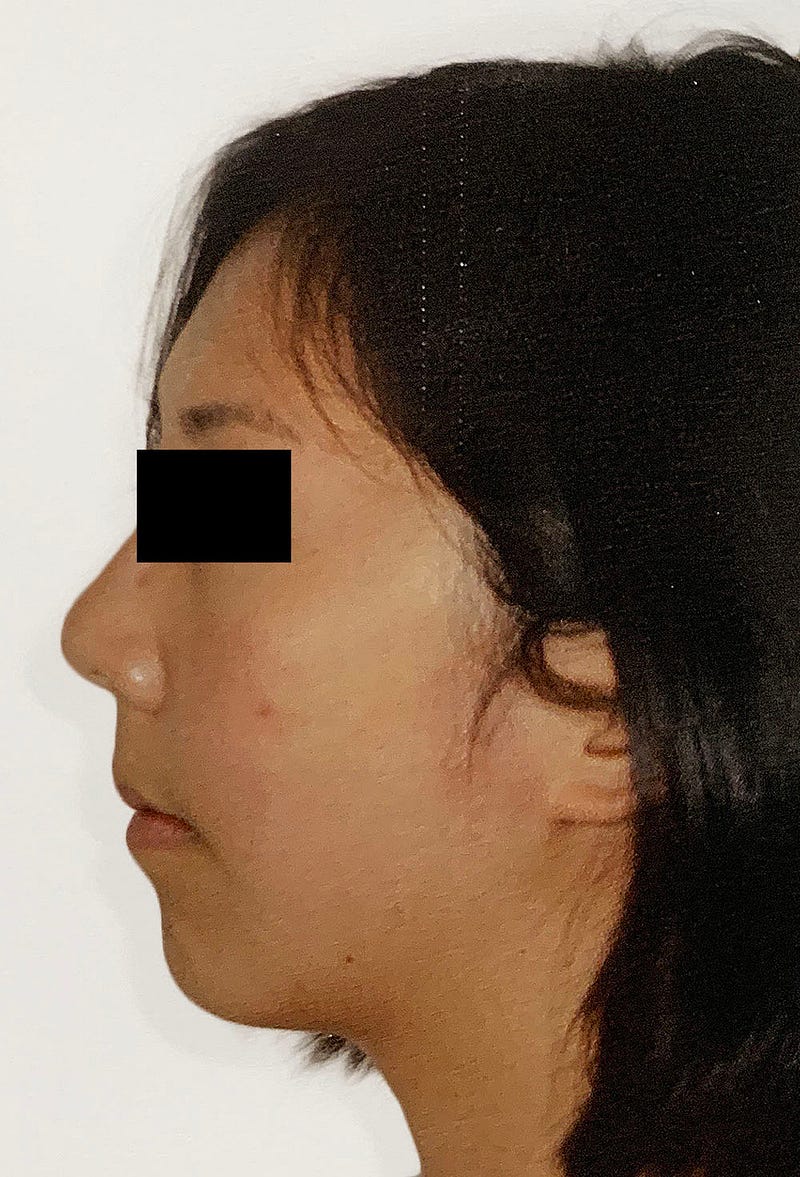
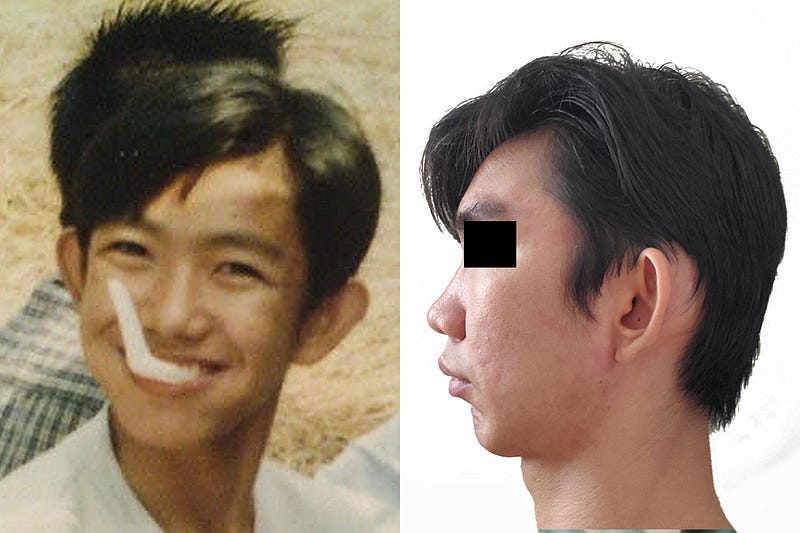
Magdalena, age 24, Chile

Only photos provided: before and after. Magdalena is currently seeking jaw surgery in an effort to restore her original face.
John, age 21, Brisbane, Australia
I had extraction and retraction Orthodontics at 14 years of age. I had a very minimal overbite and an already narrow palate before beginning my orthodontic treatment. I was happy with my smile and the way I looked and felt — but my orthodontist explained to my parents that braces and extractions were necessary. My treatment consisted of removing two upper permanent first premolars. Even as a 14 year old with no knowledge of orthodontics, I found the thought of removing healthy adult teeth barbaric — but I trusted that my orthodontist had my best interest in mind.
I wasn’t aware that these extractions would have both aesthetic and functional consequences. Within a year after having my extractions, I found that I started to develop TMJD which gave me awful pain in my TMJ when eating and sometimes even talking. For about 2 years my jaw felt ‘locked’ and I could only open it so far. My orthodontist didn’t seem worried and brushed my concerns to the side. I still have TMJ issues to this day.
While in high school, I was always an athletic guy and trained competitively for sprinting. But I found that part-way through my orthodontic treatment, exercise (specific cardio) became a lot more difficult and I could no longer train as well as previously. It’s possible that this is due to having a smaller airway from retraction orthodontics and therefore less oxygen for my body when doing high-intensity training.
On top of all this, there were many aesthetic consequences. My face and smile began to narrow, my chin became weaker and basically non-existent, and my jaws were misaligned and set-back, creating a concave side profile with little-to-no jawline. People at school that I considered friends would constantly make comments on me having ‘no chin’ and they thought teasing me about it was both harmless and hilarious — not realizing the negative affects they were having on my confidence and idea of self-worth that still heavily impact me to this day. This led me to getting a genioplasty in my first year out of high school as I thought this would ‘fix’ me and help me to love myself better — and it did help slightly — but unfortunately a genioplasty alone is not enough to fix years of orthodontic treatment. After doing more research I began to look into ways to reverse the effects of my previous orthodontic treatment. I am now in my second round of braces to prepare my teeth for orthognathic surgery to bring both my maxilla and mandible forward to open my airways and create a better aesthetic appearance.
Daniel, age 26, Spain

My name is Daniel, I live in the south of Spain. When I was 13 years old (2007), my mother decided to take me to an orthodontist due to the fact that orthodontics was fashionable at the time, and many of my friends in school were in braces. I was a mouth-breather, with a class 2 bite. The orthodontist suggested taking out 4 premolars, plus 2 milk teeth.
Once the braces began to close the spaces, all sorts of ailments developed: from sleep disorder and lack of concentration to difficulty with pronunciation to lowered self-esteem to weight loss (10 kilos), all within a matter of months. I thought all this was due to adolescence. I used to play basketball and tennis and enjoyed sports very much. After the orthodontic treatment, physical activity was hell to me. My academic performance also declined; I started to fail in subjects that before gave me no problems. I had to repeat high school twice because my brain was totally exhausted. I felt tired all day, I suffered from social anxiety and depression that was impossible for psychologists to treat, since it was not known where it came from. I started adopting sedentary habits like staying longer at home watching television series or playing video games because I didn’t enjoy going out partying at all. My social life was practically nil after that treatment.
I went to university ignoring my problem. It was only at the age of 26 that I learned that I suffered from severe respiratory problems and that my insomnia came from sleep apnea caused by the retraction of the jaws and the lack of space for the tongue in the mouth. The orthodontic work had also caused bruxism and pain in the temporo-mandibular joint. My face, which had always been round, had become elongated. When I look at the before and after photos, I am completely unrecognizable.
The only reassurance I have today is that none of it was psychological, and that there was a logical explanation behind it. That is why I no longer strive to overcome this situation by doing extreme diets, exercise or strange behaviorist techniques derived from useless psychological therapy. At this time, I am in the process of searching for an orthodontist who understands the problem because already 3 maxillofacial surgeons haves suggested that I will have to undergo orthognathic surgery to resolve this issue.
Janice, age 61, New York, New York
I’m a New Yorker who spent my childhood and teenage years growing up in England. I also spent some time living and working in Europe and went to college in Kenya. Since then I’ve had several careers in student exchange and publishing, and more recently, my own company creating press and publicity for small businesses.
As a child in the UK, I had four bicuspids extracted at the age of 9 and then braces with headgear slapped on to excruciatingly pull my jaw and teeth backwards. I was told was that my teeth were too big for my mouth, which is also what my parents were told by the Harley Street orthodontists in London who employed these extraction orthodontic procedures in 1968.

I have certainly paid the price ever since then. I am now 61 years old. I suffer from TMJ, jaw clicking, increasing difficulties breathing and getting a full breath, unable to get air for seconds, choking on food, and a collapsing jawline and neck.

The removal of 4 bicuspids at age 9 and 4 wisdom teeth at 22 has also affected my speaking voice. I tend to garble words at times and people don’t understand what I’m saying as I rush and stumble to get the words out of my stunted mouth.
For the past 12 years I have been attempting to reverse what was done to me so long ago, with different palate expanders and orthodontic work. Silly perhaps but I know that I have a nice singing voice and I know that it has been stifled because of the retracted position of my jaws. I was meant to have a big forward jaw, and together with my beautiful big teeth my natural face would have been much more striking than it currently is.
I know my parents meant well when they took me to those Harley Street orthodontists in London, England in 1968 but they inadvertently caused me severe lifelong damage.
I may be 61 today but I am still determined to do what I can to reverse things. I am in the process of seeking out further treatment to possibly reverse the terrible butchery of extraction orthodontics. My goal is to be able to breathe fully again for the rest of my life. And perhaps to finally be able to sing.
Mick, age 21, the UK

I’m a 21 year old computer science student who had upper premolar extractions at the age of 16 and braces. The procedure was not explained to me at the time, just that I had to have them out. Throughout my treatment process I noted subtle facial changes but disregarded them as I thought as the orthodontist is in a position of authority they would know best. Throughout treatment I had this sensation of my lower jaw being pulled back into my face which was rather uncomfortable but I endured it for the reasons I stated
After treatment TMJ symptoms developed and got continually worse until two years after treatment I went back to the dental office and talked about my problems. They were quick to dismiss me and tell me it’s all in my head and that there’s no scientific links to my symptoms. I went back there a total of three times to complain and plead before realizing I wouldn’t get anywhere: I complained of the reduced tongue space and clicking of my jaw. His reply was we don’t treat jaw clicking as a problem in our field.
From then on I knew that this problem was way out of my hands: it’s the curriculum that dentists are taught. The curriculum needs updating to favor airway and facial growth rather than just straight teeth. It’s quite hypocritical that jaw surgeons usually advance the jaws and orthodontists retract them. All of this has caused me extreme pain and anguish as there’s not a minute that goes by in my passing day that I’m not reminded of the mutilation that has occurred to my face aesthetically and the pain which I go through constantly. It’s definitely been detrimental to my work and social life although I continue to persevere and strive to succeed in my work alongside continuing to search for a solution to my illness.
Marina, age 52, Stockholm, Sweden
I had crooked teeth and an overbite as a teenager. When I was 22 and earned my own money, I decided to straighten my teeth. I went to a dentist who extracted my four wisdom teeth and two premolars. The orthodontic work gave me a bad bite so I started grinding my teeth. My gums receded and my teeth were worn down. Now I suffer from TMJ, painful teeth, tinnitus and poor sleep. My anxiety and stress level have gone up. That the cause for these issues is the orthodontic treatment I had has all been concluded by several dentists, so it is not anything I found out myself. Now at the age of 52, I suffer pain 24/7 and I wish I had not done anything to my teeth at all.
Sovanna, age 31, Cambodia
I was 15 when the extractions happened: 2 upper premolars + 2 lower first molars. My symptoms began at age 18. I have headaches / jaw muscles strain / jaw clicking /neck pain / swallowing difficulty/ irregular heartbeat and breathing difficulties. Today I can no longer sleep because of the breathing difficulty.
My dream was to study languages abroad and travel the world, and to have a family. I speak a few languages, Khmer as mother tongue, English, Thai, Chinese (not so good), and some Japanese. In my third year of university, I got a scholarship to study in China. I had to stay home with my mother, because of the pain. I work now online selling watches. I like this job because I do not have to meet or speak to people, and I can do it at night when I cannot sleep. I work lying down because of the neck pain. I had to quit school and now focus on learning languages myself by listening a lot to podcasts, radio, watching YouTube videos and talking to native speakers through language exchange app.
I have tried to find help since age 17. I have seen countless doctors, every dentist in Cambodia. I would ride with my xrays in my knapsack on my motorbike and stop every time I saw a sign that said “dentist”. They said the problems were in my head. I also went to Thailand.
My brother in law who is an orthodontist also did not believe me at first. But after six months he did. He tried to help me by copying techniques used in the United States to help people like me. He made his own versions of the FAGGA expansion device, and then the MSE expansion device, using Youtube videos and instruction manuals. The FAGGA pushed my teeth out of the bone, but the MSE gave me some relief with nasal breathing.
I think I need double jaw surgery or I will die from not sleeping and breathing. They do not do this surgery in Cambodia. My family has been putting aside money for double jaw surgery in the United States for the last ten years. I had a video consult with a jaw surgeon there, who I trust very much. It costs 70,000 dollars, and maybe I also need my temporomandibular joints replaced, which is 20,000 more. I just applied for my Visa. It cost 3000 dollars. I will need to wait 2 years to know if I get it. I do not know if I can live 2 years. I have just made an appointment with a surgeon in Thailand, but I am scared because I don’t think jaw surgeons in Asia work with airway issues, like the surgeon in the USA, and if the surgery does not go well, I will have more problems.
I really want this surgery to be the last treatment that I ever do and to stop thinking and worrying about my teeth. I have now spent 2/3rds of my life on this problem.
Looking back, I didn’t have a life. If I die tomorrow and have to sum up my entire life, it will be like a few minutes clip in which most of my memories are in my childhood before any orthodontics were done.
Update: Sovanna had jaw surgery in Barcelona, Spain in 2022. His surgery was botched, and he and his family are now saving for a new jaw surgery.
Lauren, age 26, Louisana
“Extraction orthodontics” when I hear this phrase, I cringe. I think of the young child whose parents were informed there was no other way to align her jaws and bite without extracting permanent teeth (two upper premolars) to treat “over jet”. I think about the upper headgear that was slept in countless nights that withheld natural growth of her upper jaw, weakening her profile. I think about waking up with cracked lips from the difficulty breathing, the dental arches being made so unnaturally narrow, that her tongue feels it has no room to rest on the roof of her own mouth. I think of jaw joints that painfully pop each day and a recent MRI that reveals onset of deterioration of her temporomandibular joints. I think about the lisp she is mocked for the aggressive narrowing and retracting of the dental arches, hindering natural pronunciation patterns of the tongue. I think of a “gift” that just keeps giving, except these gifts aren’t any that anyone deserves.
Now, as a 26 year old adult, the symptoms are a battle each day and finding a professional who truly understands how this treatment negatively affects the body is quite difficult. The headaches, jaw pain, teeth wear, difficulty breathing, painful neck, difficulty chewing, painful shoulders, pre-aging and asymmetry in the face from loss of lip support and bone loss from extractions are overwhelming. It took years to truly connect the dots after seeing several dental professionals and spent thousands on appointments, xrays, cts, and splints. I was about to pursue a career as an ultrasound technologist but the required shoulder movements alone are too unbearable to take on the career I want to pursue. As a young artist, I have to play guitar and sing in short intermittent periods of times, because of the pain in my teeth and jaw that run down my neck and into my shoulders.
You wouldn’t choose to wear shoes that were too small for daily wear, why would you choose to narrow a vital part of one’s body (the dental arches and airway) by extracting teeth? Each day, I have to choose not to focus on the pain, and choose to work toward educating others and living my life to the best of my ability, despite the health issues from my orthodontic treatment. I have hope that young dental professionals can make changes in the future.
Meg, 51, Oklahoma
My extractions took place at the age of 13, after successfully pressuring my parents to get braces on my teeth like in keeping with my desire to fit in with my junior high peer group. When my braces were removed 3 years later, I began to experience popping and clicking in my jaw joints. I was given a splint which only made things worse. At age 17, I was subjected to a second round of orthodontics, by the same orthodontist, so my jaw could “calm down.” Throughout my 20s, my parents wrote checks in the amount of thousands of dollars for appliances, physical therapists and specialists to help me while I pursued my undergraduate and law degrees. Upon entering my professional career, I decided I was done living with a mouth full of plastic splints, and was convinced to undergo a 7 hour surgery, which left me to eat out of a blender for the first year after surgery and thereafter required that I wear an appliance to eat at every meal that is not blended. I now have severe central and obstructive sleep apnea, severe nerve damage to the parotid nerve resulting in first bite syndrome, videon nerve damage, trigeminal damagem patulous (open) Eustachian tubes bilaterally and a condition known as Empty Nose Syndrome. As a result of my injuries, I’ve been adjudicated permanently disabled.
Since that fateful day in October of 1983 when my 4 bicuspids were removed I, an otherwise healthy person never having had any major health condition, have had 4 rounds of orthodontics, worn countless intra-oral devices and 4 types of headgear to work, eat, sleep and church, 6 surgeries with 27 procedures, and 3 rounds of highly painful stem cell injections. I am now 50 years old, never married, no children and with a destroyed legal career. My earnest prayer is that this story of my devastation will be made available as a cautionary tale for those contemplating the baseless and unnecessary removal of irreplaceable, precious body parts.
Patrick Zwally, age 30, New Jersey
My dream in high school/early college was to become a world-class weight lifter and personal trainer. I was an elite weight lifter for my height and weight with a bench press of near 300 lbs. I now am near 30 years old and have not lifted any significant weight since age 19.
At age 14, I made the mistake along with my parents of electing for traditional orthodontics which included extraction of 4 bicuspids and retractive elastics/braces. Halfway through treatment I noticed it became difficult to open my mouth. There would be clicking and pain in the jaw joint when I opened wide. The orthodontist said it was TMJ and it was “nothing to worry about”.
I started to have shoulder/neck/jaw/hip pain around age 19 and it progressively got worse. It was very difficult psychologically that I had to stop weight lifting then because it was more than just a passion, it was a huge part of my identity. During my 20’s I consulted with 100+ doctors/dentists trying to figure out the root cause of the pain and return to normal life.
The jaw/neck/shoulder pain (along with severe snoring) eventually took over my whole life. The situation became so dire it led me to the point of near suicide. It got to the point where I couldn’t speak for months on end because my jaw was completely locked.

I ended up having double jaw surgery and total jaw joint replacement surgery at age 28. It was a major success and did in fact have a huge improvement on my overall health and well-being.
But if I could go back in time, I would have ended my life long before the jaw surgery ever took place, knowing the horrors I was to face in the two years leading up to surgery, and the eight years prior.
Heloise, 42, France
Letter sent by registered mail to her childhood orthodontist:
Madame,
Thank you for your response to my previous letter, however you did not answer the other questions I asked:
- When in your diagnostic did you assess the space needed in my mouth for my adult tongue?
- When did you assess the possible consequences of extraction-retraction on my airways and my temporomandibular joints?
As for the signed consent form you shared with me, it is far from exposing the reality of the risks involved. I will detail below all the problems that I had and that I still have following your treatment:
The treatment you inflicted on me (extraction of premolars plus headgear) hindered the growth of my maxilla. My mouth is the same size as when I was 11, as confirmed by the dental molds that you kindly sent me. My jawline was already initially narrow due to thumb sucking and instead of solving the problem, you amplified it.
- The comparison of the before/after x-rays shows the narrowing of my airways due to the recession of both jaws, the reduction in the space available for my tongue, and the flattening of my face that happened during treatment..
- My mandible is “blocked” backwards due to my maxilla being too retracted. You should have done expansion (a technique that has existed since the end of the 19th century…) to allow all the teeth, including the impacted canine, to position themselves correctly. You did just the opposite.
- The breathing difficulties were immediate, although I only realized recently that they were the consequence of your treatment. In middle school, I suddenly had trouble running, I just thought I had become “bad at sports.” Today, I suffer very rapid shortness of breath at the slightest effort and obstructions of my airways during sleep.
- These breathing difficulties are linked to the lack of space for the tongue. I cannot keep my tongue pressed against the palate, which also causes atypical swallowing.
- Posture problems and back and neck pain have resulted from the extended head posture adopted to clear my airways.
- I also realized a few years after the end of treatment that I was suffering from bruxism. Dentists at the time told me I was too stressed. I now know that the bruxism is linked to my narrow airways.
- The retraction of the maxilla caused my mandible to move back, in an unsuitable position (as if stuck backwards), which triggers TMJ pain. I also once had a lot of jaw “clicking”, which has fortunately disappeared for the moment after more than a year of osteopathic work.
- Finally, the restriction of the growth of the jaw has caused a flattening of the face (very visible on the x-rays). I therefore suffer from, in addition to all these health problems, the aesthetic consequences of the treatment.
Since the age of 20, I have spent thousands of euros on osteopathy, fasciatherapy, dental splints, and various consultations to try to put an end to pain and other problems, obviously only obtaining temporary relief. Today, the solution proposed to me to resolve the problems consequential to your treatment is orthognathic surgery: a heavy, painful surgery which is not without risk (in particular risk of damage to the facial nerves and dental necrosis). I will incur thousands of euros in expenses since this surgery must be accompanied by orthodontic treatment which is not covered by social security.
You therefore mutilated me and put my health in danger through inappropriate treatment which ruined my life.
I am probably not the only one in this case, but it is very likely that most of those affected will never find the cause of their problems, since for my part, it is only this year, after more than 25 years after the end of my treatment and almost as many years of medical wandering, that I found out the cause.
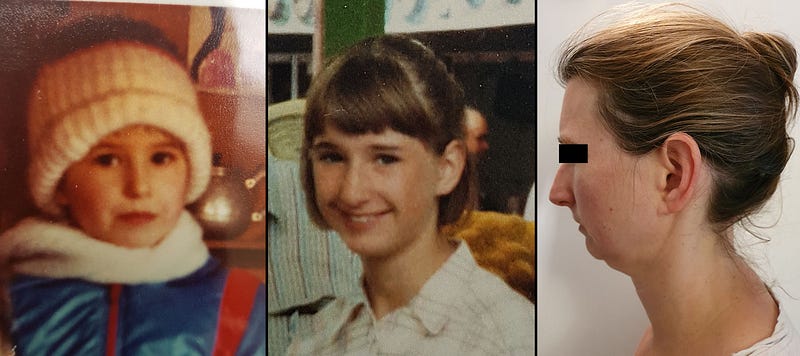
Victoria David, 37, UK
As a child, I had a fairly symmetrical forward grown face and wide jaws. I had good body posture and was quite active, healthy and happy. Today this is no longer the case.

In my teenage years, my lower incisors became crooked. I went to an orthodontist to straighten them. He proposed Premolar Extraction/Retraction to my parents and me. We questioned why four healthy teeth needed to be extracted if only my bottom incisors were slightly crooked and were told that otherwise all my teeth could become misaligned. Scared that all my teeth were going to become crooked if my teeth were not extracted and reassured by the fact that my mother had also had her own teeth extracted/retracted in childhood, we proceeded with treatment.
Looking back, I strongly feel that I would have benefitted from an expansion orthodontic treatment. Not only would this have been more aesthetically pleasing but more importantly I would be much healthier today.
During the Retraction phase of treatment, I noted that my face looked like it was changing. The Orthodontist insisted that I was imagining it, and I was left feeling like a naive teenage child. I felt embarrassed and did not dare question him further as he, being a health professional, must know better than my teenage self.
At the end of the treatment, my peers began to ostracize me because of my new dished in smile and would mock my face. I had never had anyone mock my teeth, smile or laugh when I was a child. This new negative response from others made me aware how recessed my face appeared to others and that I no longer had my pleasant wide smile. My childhood self would not have imagined growing up to experience such depression.
I began gasping for breath during sleep which would wake me. My partner brought it to my attention later, when we first started dating, that I stop breathing for periods in the night which still causes him concerns. I also experience dizzy spells where my eyes will glaze over until my sight and breath returns, almost like vertigo. I struggle to do cardiovascular exercise as I get out of breath quickly and my chest feels tight.
By my early twenties, I observed that my face had aged prematurely and my skull had narrowed. I no longer looked youthful. It was strange having a young healthy body with a sickly looking head. I could not understand why my jaws had narrowed, retracted and twisted when for the first eleven years I had a symmetrical face and forward growth. I was deeply unhappy with the changes to my appearance and body.
I became suicidal and began to self harm.
Today I wish I weren’t so tired all the time and that I could return to looking regular rather than dished in. A lot of today’s Instagram generation wants to look like some unattainable beauty whereas I personally would love to look healthy and regular to blend in the crowd so to speak. My head is narrow and concave, my eyes are down-turned and my jaw is blended with my neck. My body posture is poor due to Forward Head Posture from hanging my head forwards to breathe, and I have a Dorsal Hump at the top of my spine. My skull is noticeably asymmetrical, and my Tempormandibular Joints are also uneven.
There is little room in my mouth for my tongue. I have the intermolar width of a child. I have a low hyoid bone which has left me with a double chin in spite of me having a slim physique throughout my adult life. I also have to tilt my head back and lift my chin for others to see me smile or speak because my line of bite is no longer aligned with my line of sight. However, when I tilt my head back to speak I am self-conscious as my nostrils are exposed to those I am talking to and my ears appear low set.
Not only is this experience depressing, it is isolating, as those in my inner circle dismiss me and deny the physical changes. So do the doctors I have consulted with. One orthodontist denied that PER had caused my skull to change, suggesting that people of European origin by nature have narrow skulls and that our American cousins naturally have wider skulls.
It is an isolating experience, when your inner circle denies the changes to your appearance and health, however others outside your circle mock the unpleasant physical features you are left with. It is painful to be gaslit by loved ones and by Health Professionals who deny what you physically experience and the changes to your own body.
Fortunately, some friends can see the changes from looking at my childhood photos, and a Therapist confirmed she also sees the physical changes. She also told me that I am not the only person to seek Therapy for PER consequences in the UK. Another Therapist advised me that those who are not listened to by their loved ones are more likely to have Mental Health issues. She added it is important for those who experience trauma that they are not only listened to, but heard.
For the longest time I believed it was just me and I was unlucky, until I found groups of people on online forums reporting the same experiences as me. It is these groups that have educated me on treatments that can undo some of the damage. However, there are no treatments to reverse PER damage in the UK and I am not financially in a position to have treatment. My partner has suggested I set up a crowdfunding campaign so I can get help to begin my journey into undoing the damage. It is my hope to get MSE palate expansion in Europe as this procedure is not available in the UK, followed by maxillary remodeling using deep MOPS with Dr Daniela Storino in Brazil.
America’s online dictionary Merriam-Webster defines the word Retract as “to draw back or in” with the intransitive verb “to draw or pull back”. The Oxford dictionary defines Retraction as “the action of drawing something back or back in”. Given this definition and that the Treatment is named Extraction/Retraction, how can orthodontists dismiss that the treatment retracts when the word is in the procedure’s name? How can they say that our negative outcome is from genetics? We are all from different corners of the globe, from different races and from completely varied genetic lineages. PER treatment has the same consequences for all of us regardless of our genetics.
If orthodontists do not believe us, then why not have they not investigated all of us as individuals to prove us wrong? Can any medical professional explain why my skull has narrowed, my chin has retruded, my nose has twisted and my ear and eye have dropped down on one side?
Answer our questions and prove that we are wrong if you disagree with our claims. Investigate this deeply if you do not agree PER has affected our health.
By speaking up, I and others do not want to pose a threat to the Orthodontic profession. We want to simply ask them to stop PER treatment, then progress into expansion techniques as well as treatments to help those affected by PER. Surely expansion treatment would benefit patients and create healthier future generations.
I would not wish for anyone to experience the changes to their health and appearance like myself and others who have had PER.
Amit, age 49, India
I had 4 second premolar extractions at age 29. I now have temporomandibular disc displacement, C5-C6 displacement in my cervical spine, pain in ears, and brain fog. Put an end to my career in finance. I remain single and have no career. I took to yoga and spirituality. Persevered with finding a solution to my iatrogenic disorder, but to no avail. I am now a yoga teacher and writer, and also work in my family farm and rental business. I sing out to the lord: “Hey Govind, hey Gopal, I am losing my battle, please help.”
Sarah, age 30, New York City
When I was in my early teens, I had 4 premolars extracted as my orthodontist told my family that I didn’t have enough room for my teeth. I then entered the world of braces, wearing them for nearly 2 years, followed my headgear, retainers, and then wisdom teeth extraction.

My face looked very thin afterwards. I just believed it was because my face was “thin”. I never thought much about it. I was a child. When I was in my early 20’s, I went to the dentist and was diagnosed with TMJ in my right joints. I lived with it until it became progressively worse. In my late 20’s and early 30’s, I was also very unhappy with how I looked and had (and still have) trouble feeling confident with myself. I went back to an orthodontist and he proposed Invisalign to straighten some teeth. The Invisalign treatment tipped my situation over the edge. My face caved it almost immediately. People asked if I was okay and if I was losing weight. My cheeks became flat. My TMJ progressed. I began wearing a splint, a gentle SOMA palate expander, with no relief.
Today my headaches consume my entire head, eyes, ears, and neck. My c1 and c2 vertebrae are compressed. I am in pain everyday. I sleep in pain and wake up in pain and need coffee to even feel like I am alive. At 38, I am single and feel alone in this journey. I have utterly lost my self confidence and worry I will never marry, feel beautiful, have children (as my oxygen levels are so low and I am constantly in fight or flight mode), or generally ever feel like I can fully enjoy this life. When I look at other people just enjoying their lives, at restaurants or laughing with friends, I feel left out, like the world is going on without me.
It is a hard awakening to realize that I am a victim of childhood extractions. It isn’t fair.
I am doing what I can to get better. I am currently working two jobs to pay for eventual reversal treatment, and see doctors and orthodontists every week searching for a solution, sometimes traveling to other states for the consultations. I have been proposed double jaw surgery as well as palate expansion methods, and so many different options that I am unsure what direction to go. I fear that any wrong move can make the TMD worse and that my body won’t be able to handle surgery. My hope is that the right people will come to me who will guide me to the right decision. I feel very lucky to have found a physical therapist, an osteopath and a retired periodontist who offer some relief for the pain.
Sarah recently learned that she needs Total Joint Replacement (TJR) in addition to double jaw surgery.
Ronald Ead, age 30, Boston
I had extraction orthodontics at age 12. Chronic migraines and neck pain began the year I finished the treatment. I pursued orthodontic reversal techniques starting at age 26. Over the last four years, I have tried the following reversal techniques, in this order: Acrylic Schwartz expanders, frenectomy, AGGA/CAB, and MSE.
In 2017, I created a website and YouTube channel entitled JAW HACKS to document my experience with the AGGA appliance and with migraine nerve decompression surgery, as at that time there was little information about either treatment online. The content now includes research in various adult orthodontic expansion appliances and treatments. My blog gets 4300 unique viewers per month, and my YouTube channel has had 434,000 views.
A word of advice to people who are reversing their premolar extractions: you should know that reversing extractions takes a tremendous amount of motivation as well as perseverance. It is important to remain mentally strong when complications arise. The most important thing is to go into the reversal process with knowledge of the landscape and a healthy amount of cynicism toward treatment providers. Navigating the world of extraction reversal is a minefield. I hope my content helps people navigate through it safely.
_________________________________________________________________
Some of the patients by request have used their real names; the majority have used pseudonyms.
Addendum by the Author
Many patients (including the majority of the ones above) are now in the process of trying to reverse their extraction/retraction due to health and/or aesthetic consequences. Extraction “reversal” is a growing new specialty in orthodontics (especially in the United States). It requires a minimum of 3 years of treatments and usually includes some combination of orthodontic work, palate expansion, maxillo-facial surgery, bone grafts, gum grafts, splints, dental implants, osteopathic treatment and/or myofunctional therapy. The outcome of “reversal” (a misnomer, as the extraction/retraction cannot be “reversed”) is unsure and can lead to more damage such as gum recession, root resorption, teeth loss, facial asymmetry and — with maxillo-facial surgery — nerve damage and permanent numbness. The most difficult part of reversal that patients report is finding an orthodontist willing to recognize their condition and capable of directing the treatment. Another challenge is the cost. Costs for reversal treatments can reach up to 90,000 dollars (or 250,000 dollars, if total jaw joint replacement is needed), most of which is not covered by insurance, since Orthodontic Extraction/Retraction Syndrome (OERS) is currently not recognized and has no diagnostic code.
Support Groups for Patients Damaged by Premolar Extractions:
- Extraction Orthodontics Reversal — All Countries
- Victims of Extraction/Retraction Orthodontics — UK/Ireland
- Victims of Extraction/Retraction Orthodontics — Australia/New Zealand
- Victims of Extraction/Retraction Orthodontics — USA
- Victimes des extractions prémolaires et de l’orthodontie (France)•
- Extraction Reversal — Asia Community
- Scandinavian Premolar Extraction Support Group — Telegram
- Victims of Orthodontic Extraction/Retraction - India group
Today the majority of orthodontists claim that premolar extraction/retraction is without risk.






{kind=link}