
Our Best Insomnia Medications Don’t Even Work on Sleep
Orexin blockers no longer fly under the radar

Some of our best sleep agents have been on the market for a decade, but many people remain unaware of them. Dual orexin receptor antagonists (DORA) like Belsomra, Dayvigo or Quviviq work dramatically differently than other sleep medications. They don’t even promote sedation.
Clinically, cognitive behavioral therapy approaches to insomnia (CBTi) are always the first choice option for sleep problems. CBTi is as effective as any medication, without the side effects. But DORA drugs powerfully improve sleep for many, without many of the drawbacks of sedating agents. DORA drugs have been underutilized, but exciting new research on dementia may soon prompt many more people to start taking these medications.
Oh really? What’s Orexin?
Chances are you haven’t heard of the neurotransmitter orexin. Only about 70,000 neurons make orexin and use it to signal other cells in the brain. That’s less than one out of every million neurons! But that actually means that the scale of the orexin system is pretty similar to that of serotonin (which is four times larger) or dopamine (ten times larger). Like those better known systems, the cell bodies of the orexin system exist in a tiny part of the brain (in this case the lateral hypothalamus) but send projections all over the brain, powerfully influencing neural activity in many locations.
Not only is the orexin system numerically tiny but it was also discovered a half century after we learned about serotonin, dopamine and norepinephrine. Independently, two different groups stumbled upon orexin and published their findings in 1998.
One group was studying receptor systems for which no neurotransmitter had yet been identified. They called their molecule “orexin” for the Greek word for appetite. (Anorexia comes from the same root.) They knew that the lateral hypothalamus was involved in regulating feeding behavior.
The other group was examining genes that were expressed in the brain, whose function had not yet been recognized. They called their molecule hypocretin because the cell bodies were in the hypothalamus, and the protein neurotransmitter structurally resembled the digestive hormone secretin. Once scientists realized that orexin and hypocretin were the same molecule, they agreed to a confusing compromise. They’d refer to the gene as hypocretin, and the protein made from it orexin. Over time, more and more neuroscientists use orexin to refer to all aspects of the system.
Researchers identified two forms of the orexin protein, imaginatively named Orexin A and Orexin B. They identified two types of receptors, imaginatively named ORX1 and ORX2. But to add some complexity, Orexin A binds equally well to ORX1 and ORX2, while Orexin B binds ten times more strongly to ORX2 than ORX1. The two receptor systems have somewhat different distribution patterns in the brain. Some research suggests that ORX2 is more intimately connected with wakefulness and arousal.
Within a year of orexin’s discovery, narcolepsy researchers jumped into the field. Doberman Pinschers that had a genetic predisposition to falling abruptly asleep when they became excited had a mutation for the gene coding for orexin. Orexin deficiency was then found to be a common cause of narcolepsy in dogs and in humans. This triggered a flurry of research into orexin’s role in sleep and arousal.
Orexin plays a major role in both initiating and maintaining arousal and wakefulness. We have two distinct and opposing systems in our brains, one of which controls sleep, and the other arousal/wakefulness. Usually, when one of these systems is active, it sends signals to shut down the other system. But sometimes this mutual inhibition fails, and both systems are vying for control, in conditions like narcolepsy, or in sleep-deprived states when dreams may start to intrude before one actually falls asleep.
In addition, the circadian clock sends important, regulatory signals to the reciprocal sleep and arousal systems.
We have at least two arousal/waking systems. When you are startled awake by your alarm clock, other loud noise, a bad dream, or a kick from your bed partner, you’ve engaged the sympathetic nervous system’s flight or fight response. But when you wake up spontaneously, after a good night’s rest, that’s the more peaceful orexin system starting your day.
Orexin research rapidly expanded beyond the arousal/wakefulness system. Building on orexin’s role in regulating feeding behavior, orexin neurons integrate several channels of information about the biological state of the body (circadian time, blood pressure, nutritional status, hormone levels) and then send signals to other parts of the brain to drive feeding and other reward-seeking behaviors. Orexin plays a role not just in eating regulation and disorders, but also in drug seeking and addiction.
Distinct from its role in simple arousal, orexin regulates attention, and perhaps other executive functions of the brain. Orexin also plays a role in setting what neuroscientists call “hedonic tone” or the ability to feel pleasure. Part of the misery of depression arises from chronically low hedonic tone. But low hedonic tone also plays a role in those with ADHD, who seek out excessive stimulation because they otherwise feel constantly bored.
The first orexin drugs were agents that bind to orexin receptors and activate the system. Modafinil (Provigil), and later armodafinil (Nuvigil), were designed to treat narcolepsy, but also promote alert wakefulness in a number of other conditions that cause daytime sleepiness, including sleep apnea, shift work, sleep deprivation, and sedation from medications. Some call them non-stimulant stimulants because they act primarily on orexin, rather than the sympathetic startle system. Modafinil also improves symptoms of ADHD and can help alleviate depression.
Getting Back to Sleep
One of the most significant sleep medicine findings of recent years is that the vast majority of people with insomnia don’t have anything intrinsically wrong with their sleep system. Yes, you read that right. Insomnia is almost always a failure of arousal systems to turn off, rather than a sign of a broken sleep system. An ideal sleep agent would shut off arousal, clearing a path so that your intact sleep system can metaphorically land on your pillow and lull you into the land of dreams.
On paper, the DORA drugs, by blocking orexin receptors, make ideal sleep agents. As outlined in the chart below, we now have three of these agents available. Their generic names sound like a clan from Game of Thrones: Suvo, Lembo, and Dario Recant. And make sure that you don’t confuse Quviviq with qiviut, the extremely soft and durable underfur of the muskox.
Although there are some differences among the members of this class, overall they are very similar to each other and distinctly different from other sleep agents. While most people will likely respond similarly to any DORA, some individuals may sleep better with one particular agent.
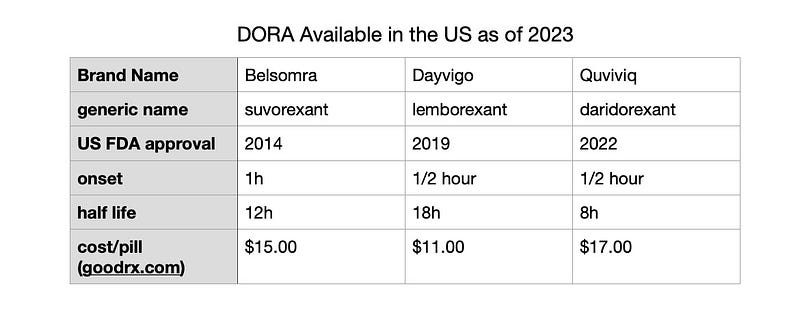
Belsomra has been ringing up more than $300 million a year in sales. That’s actually been a disappointment, representing just hundreds of thousands of users, in a country with tens of millions of people suffering from insomnia. Why the discrepancy between expectations and sales?
Almost all of the sleep medications that pre-dated the DORA drugs are sedatives. Sedatives reinforce the signal to sleep until it overrides and shuts down the arousal system. Sedatives work, even though they are piling on to an intact sleep system, rather than targeting the real problem of arousal systems that are not turning off.
Sedatives can provide a reassurance of sleep when they knock you out. If you’re accustomed to feeling stupefied by your sleep medication, you may feel disappointed that DORA provides only a muted version of this. Any anxiety that arises from not feeling knocked out can then further activate the arousal system. Many people looking for an “instant knockout”, give up on their DORA medications too quickly.
Most non-DORA sleep agents bind to sites on the GABA-A receptor. GABA is the brain’s major inhibitory neurotransmitter. Barbiturates were among the earliest GABA-A agents to be used for sleep. They sedated people, but also had a high potential for addiction. They caused death at high doses because they also suppressed respiratory centers in the brain.
Benzodiazepines, drugs like Valium (diazepam), Halcion (triazolam), Ativan (lorazepam), ProSom (elprazolam), Restoril (temazepam), and Klonopin (clonazepam) represented the next wave of sleep agents. Although some benzodiazepines were marketed for anxiety, and some for sleep, all of them were effective for both conditions. Benzodiazepines differ among themselves by how quickly they start working, and how long they last. Some that were marketed for sleep had half-lives close to a day, meaning they contributed significantly to next day sedation.
Benzodiazepines are far safer than barbiturates, because even large overdoses usually don’t suppress breathing. However, combining benzodiazepines with even moderate amounts of alcohol (another agent working on GABA-A) can shut down breathing and result in death. With benzodiazepines, muscle relaxation and anti-anxiety effects complement the directly sedative effects, increasing their power in promoting sleep, but also adding to potential problems.
Benzodiazepines, in a dose-dependent way, cause problems with coordination and reaction time. They can impair one’s ability to know that they are impaired. Most people develop tolerance to any of the GABA-A agents, needing higher doses to get the same effect, and a significant proportion of people develop addiction to these substances.
Benzodiazepines also produce rebound insomnia. After just a night or two of use, it is measurably harder to fall asleep for the first few nights off the drugs. Benzodiazepines contribute to serious car accidents, and to falls in the elderly. They can acutely impair memory. Several large studies indicate that prolonged, regular use increases the risk of dementia.
The discovery of two types of benzodiazepine receptors led to the development of the next generation of sleep agents, the Z-drugs. Zolpidem (Ambien), zopiclone (Lunesta), and zaleplon (Sonata) work primarily on the benzodiazepine sleep receptor. They have less impact on the other benzodiazepine receptor, reducing the likelihood for muscle relaxation, memory problems and addiction compared to the full benzodiazepines. Both full benzodiazepines and Z-drugs can distort sleep, decreasing the percentage of REM sleep, and contributing to rare occurrences of sleepwalking or sleep eating.
The DORA agents represent a significant departure from the parade of sedating, GABA-A acting sleep drugs. Unlike other agents (and similar to CBTi) the DORA agents work better for sleep the more you use them. Their potential for addiction appears significantly lower than that of other agents. They don’t suppress respiration. So far, problems with sleep walking and other anomalies appear less frequent than with benzodiazepines or Z-drugs, although rigorous studies of these rare adverse effects are hard to conduct. DORA agents reduce the time to fall asleep, improve total sleep time, and improve the amount of REM sleep.
Dementia to the Rescue?
DORA agents work for sleep. But their lack of powerful sedation, and their high costs have hindered sales. New studies of dementia may change their market share.
Poor sleep is strongly associated with the development of dementia years later. This association complicates research into whether benzodiazepines and Z-drugs increase the risk for dementia. It can be tricky to decipher whether those sleep agents really increase dementia risk, or whether we are just detecting the effects from underlying or under-treated sleep problems.
The recently discovered glymphatic system flushes toxins, including broken proteins, from your brain only during sleep. Not only that, it works only during sleep at night time. The chemical hallmarks of Alzheimer’s disease are the accumulation of two aberrant kinds of proteins: neurofibrillary tangles from tau proteins within neurons, and beta-amyloid plaques in the extracellular spaces. Without adequate sleep, these toxic proteins accumulate and cause inflammation, neural destruction, and further damage to brain circuitry.
Studies in mice genetically prone to developing dementia show that when orexin is inactivated, either through DNA modifications knocking out the gene, or by administering DORA, brains accumulate less beta-amyloid. A recent study in humans showed that just two nights of Belsomra produced measurable decreases in toxic forms of both the amyloid and tau proteins in cerebrospinal fluid. Whether this resulted from improvements in sleep, or a more direct biochemical effect, remains unknown.
Many people in modern society take pride in their self-inflicted sleep deprivation. Almost nobody humble brags about mild cognitive impairment or full blown dementia. Lowering the risk for dementia may be a more palatable selling point for DORA rather than their demonstrated benefit of treating insomnia.
Improving sleep leads to a decrease in daytime symptoms for a variety of mental health conditions, including depression, bipolar disorder, substance abuse disorders and ADHD. Whether DORA will provide additional benefits for the treatment of these conditions, beyond those accruing through improved sleep, remains a topic of intense interest and research.
DORA provide decent help with sleep problems with minimal side effects. We don’t need to feel sheepish if these medications become truly popular because of other benefits they have. It shouldn’t get your goat, and you shouldn’t have a cow about it. It doesn’t make their use as effective sleep agents full of bull. Things are often more complex than they appear. Good sleep medications may turn out to be effective anti-dementia drugs. After all the closest relatives of muskoxen are sheep, not cattle.





