
THROAT CANCER | CANCER JOURNEY | MEN & HPV CANCER
My Husband’s Journey with Throat Cancer
From diagnoses to treatment

Since my husband is now preparing for radiation treatment for prostate cancer, I’m reflecting back to 10 years ago when he dealt with throat cancer.
January 10, 2013, my husband and I visited our family doctor for his blood test results and a checkup on the mild sore throat he’d had for months. While examining him, she discovered he had swollen lymph nodes on one side of his neck.
The doctor immediately suspected cancer.
Possibly in the salivary gland. She set up an ultrasound appointment at the local community health centre.
Ultrasound results were unclear. The doctor set up a CT scan at the same health care centre and referred my husband to an ENT (ear, nose, and throat) doctor to have a biopsy performed on his lymph node.
January 28, 2013, we went to a nearby city for the ENT doctor appointment.
The doctor viewed my husband’s throat with a scope. It was then the doctor saw a lesion on the base of my husband’s tongue. “Throat cancer,” he said. “You’ll be lucky to live 5 years.”
He performed a needle biopsy from the larger of two swollen lymph nodes.
The next day, my husband’s neck swelled, and he had to go to the emergency department.
February 2, 2013 — The biopsy results were unclear. The ENT doctor performed a second biopsy on the smaller lymph node.
Feb 11, 2013, the second lymph node biopsy results came back with no clear results. The ENT doctor referred my husband, Mike, to another doctor to have a biopsy of the base of his tongue.
Two days later, on Feb 13, we were at the hospital to meet this new doctor. An otolaryngologist (OH-toh-LAYR-in-GAH-loh-jist) for head and neck surgery. An otolaryngologist is often called an ear, nose, and throat doctor, or an ENT for short.
They allowed me in the room to watch.
First, the doctor sprayed Mike’s nostrils and the back of his throat with a numbing agent while Mike sat upright in a chair. The doctor then passed a flexible tube (endoscope) through one nostril to the back of his throat and base of the tongue. An instrument was then passed through the tube to get a tissue sample of the lesion on Mike’s tongue.
This doctor also took another biopsy of the larger lymph node.
February 21, 2013, the biopsy results were positive for cancer.
HPV (Human papillomavirus) is the most common sexually transmitted infection (STI). It can cause throat and mouth cancers which are less aggressive than cancers in these areas that are unrelated to HPV.
The virus can lay dormant in cells for years. If the body doesn’t clear it. Sometimes, it causes cancer. Once that happens, the cancer can be relatively slow-growing. It can take months to become noticeable — most people don’t notice it until it becomes a lump in the neck.
Over 90 percent of sexually active men and 80 percent of sexually active women will be infected with HPV in their lifetime. — from the CDC goverment site on HPV
It made me wonder if I’d passed the virus on to my husband or if a previous girlfriend had.
His mother had died at age 42 of cervical cancer. I wondered if her cancer had been caused by HPV.
The most common types of HPV-associated cancer are cervical cancer for women, and oropharyngeal (mouth and pharynx) cancer for men.
These cancers, often caused by these viruses, are HPV-associated cancers and include cervical, vaginal, vulvar, penile, anal, rectal and oropharyngeal (mouth and pharynx) cancers. — from the CDC goverment site on HPV
March 5, 2013, was a significant date for our family, as it was our son’s 30th birthday, just two days after our daughter’s 31st birthday. We met with the ENT surgeon and the radiation oncologist to discuss treatment options and a plan.
The resident who first examined my husband was quick to say the first line of treatment would be to cut out the cancer. We sat stunned.
The possibility of removing most or all of his tongue was terrifying.
Early diagnosis and treatment may lead to better outcomes. For tongue cancer, the NCI (National Cancer Institute) calculates the five-year relative survival rate as 84.5 percent for localized, 69.9 percent for regional and 40.8 percent for distant, with a combined rate of 69.7 percent for all stages.
Patients with HPV-positive throat cancer have a disease-free survival rate of 85–90 percent over five years. This is in contrast to the traditional patient population of excessive smokers and drinkers with advanced disease who have a five- year survival rate of approximately 25- 40 percent.
After the resident left the room we met with the radiation doctor.
His recommended treatment was to first try radiation before surgery to see how successful it would be. Surgery for this doctor was the last resort.
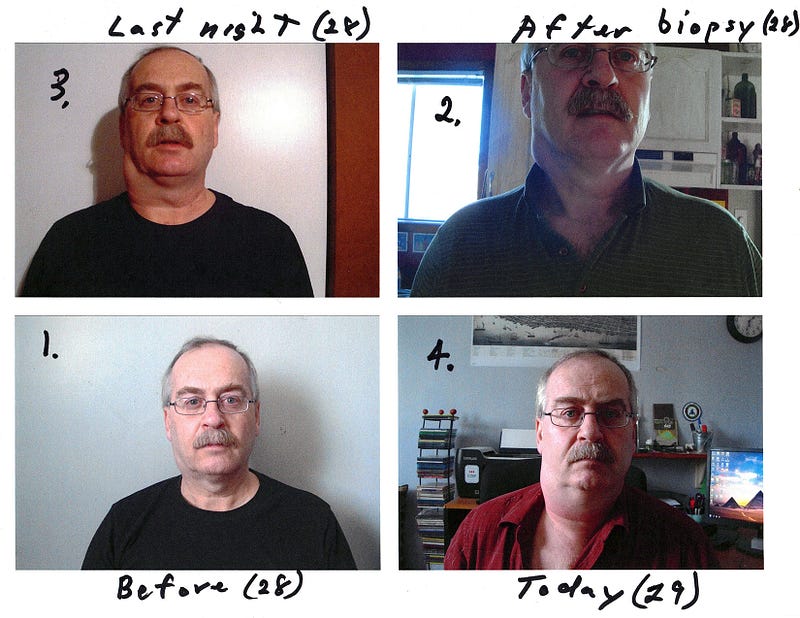
He explained to my husband that radiation might destroy a part of his mustache hair and that his skin in that area would become very sensitive. He needed to switch to an electric razor for shaving during treatments.
My husband had never gone without his mustache since a young man. But this line of treatment sounded much more positive.
Finally, the doctor overseeing the resident came in and he agreed with radiation as the first line of treatment.
Surgery, he told us, would be drastic and life-altering. Mike would most likely end up unable to eat or speak. Life as my husband knew it would be over.
My husband later said to me he’d rather die than end up that way.
March 12, 2013, we met with another doctor to discuss chemo treatment. She explained that chemo was not as effective for this type of cancer, but that the choice to do it was more for peace of mind than for its benefits. Patients did it so that if the radiation was unsuccessful, they could feel they’d done all they could.
‘Do all he could’ applied to my husband’s way of thinking as well.
Successful and unsuccessful took on a whole new meaning. One of life and death.
March 15, 2013, we went to an appointment at the hospital for the manufacture of a mask to hold his head in place while receiving radiation. He had a CT scheduled, and they got him in for an unscheduled MRI.


Hospital appointments took over our life.
March 20, 2013–-Mike had a PET scan at the VG Hospital despite the snowstorm earlier that morning.
March 26, 2013–-in the morning we attended a 2-hour Chemo Education session at the hospital.
Mike saw a prosthodontic dentist in the afternoon to do a pre-radiation screening. He would keep a check on my husband to deal with any possible damaging effects of the radiation — potential problems to his jaw or teeth.
A specialized dentist would see my husband regularly for the rest of his life.
Later that afternoon, it was off to another blood test required for the chemotherapy doctor.
The first chemo was on April 15, 2013, along with the start of radiation therapy.
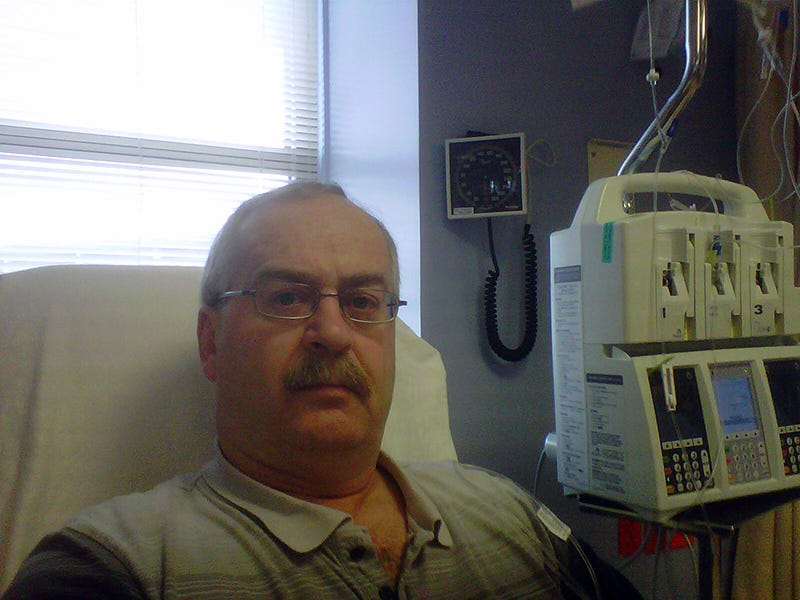
I sat beside my husband in the hospital as he received his first chemo dose.
At home, he took prescription drugs to prevent nausea and vomiting.
April 16, 2023, the next day, I went in with Mike to receive his first of 3 days of IV fluid after chemo to help prevent damage to his kidneys from the chemo drug. Cisplatin (siss-pla-tin) was the chemo drug administered. It’s the generic name for the trade name drug Platinol. Administered through a vein intravenously.
Later that day, he experienced shortness of breath when walking up a flight of stairs in our home.
The next day, Mike went to the hospital for his second day of IV fluid.
By then Mike had shortness of breath, pressure, and discomfort in his chest. She informed the chemo doctor.
The chemo doctor examined him and had him transported by ambulance to another hospital to have his heart checked.
I’d gone along in the ambulance and stayed with my husband while we waited for test results. They found no issues with his heart.
We spent the entire day at the hospital.
Afterward, we walked several blocks to the other hospital to our car.
The doctor at the hospital had prescribed a steroid medication, a beta blocker Metoprolol, and nitroglycerine to help ease his chest discomfort.
At home the next day, Mike’s temperament changed. He became irritated, angry, and aggressive. He stopped taking the steroid.
Also while at the hospital, while getting his heart checked out, Mike mentioned he was experiencing a grey, translucent spot centred in his right eye vision.

In April Mike had his first dental check-up since radiation treatments began.
Then it was back to the cardio department for an ECG, and Stress Test. Everything checked out fine and no further treatment for his heart was required.
May 01, 2013, the chemo doctor told my husband he’d receive no more chemo. The risk was too great. He had gained five pounds in one day from the fluid they’d given him to prevent kidney damage. That fluid had affected his heart.
Mike saw a specialist in the eye care centre at the hospital where they tried to figure out what was going on with his vision. He had a visual field test and a cornea exam.
Doctors couldn’t figure out what was happening with his eye. But they suspected it related to the chemo treatment. No one had any idea if it would get better or become a permanent part of his vision. (Within the year it resolved itself).
During treatment, Mike saw an oncology dietitian about eating difficulties and the need to maintain weight.
Eventually, as his treatments progressed, he could not even eat soup and needed to depend on a liquid diet of Ensure or Boost.
Ensure and Boost are nutritionally similar but not in texture.
In the later stages of side effects from the radiation, Mike could not drink the thicker Ensure and had to switch to the thinner consistency of Boost.
Mike was also provided with a prescription for Magic Mouthwash which contains lidocaine to numb the mouth and throat to prevent pain.
If he could no longer tolerate anything by mouth, the medical team would pass a nasogastric tube (NG-tube) through his nose and into his stomach.
Throughout May there were many appointments with various doctors.
Radiation treatments ended on May 28, days before his 59th birthday.

His radiation oncologist only prescribed Hydromorphone tablets for Mike’s pain. When he took a dose, his breathing slowed and often stopped, which frightened me. I feared he might die.
Something I just learned while writing this article is that hydromorphone is not the same as morphine. I had always thought it was. Apparently, it’s much more potent and can be much more dangerous if taken inappropriately. So do not confuse hydromorphone with morphine.
June 17, 2013, Mike saw his family doctor for prescription renewals. She specialized in pain management and changed the drug from the one he was on to Hydromorph Contin, and told him to only use the hydromorphone for breakthrough pain. She told us that hydromorphone was not good as a primary source of pain relief.
Again, as I researched this drug for this article, hydromorph Contin can go under the brand names: Dilaudid and Exalgo.
This change in drug made all the difference in my husband’s life. No longer passed out in a drug-induced, barely breathing sleep, he could remain awake and function. His quality of life improved.

July 04, 2013–Mike had a PET Scan to determine if radiation had destroyed the cancer.
Weeks later Mike saw both the radiation and ENT doctors for the PET scan results. The cancer on the stem of his tongue was gone, but it still showed hot spots in the lymph nodes on both sides of his neck.
It was then determined the PET scan had been performed too soon after radiation had stopped and the results could be false positives. The PET scan should happen 8 -10 weeks after radiation treatment stops. They’d done his just 5 weeks after radiation ended.
Another PET scan was booked for September.
Throughout August and September, our family doctor weaned Mike off of pain medication.
September 26, 2013, my husband’s PET scan results showed he was cancer-free!
He had scans every 6 months for the first two years and then switched to annual scans. After 5 years he remained cancer-free and checkups stopped.
Radiation destroyed the one section of his mustache and he decided for the first time in his life to shave it off and keep it off.
In May of 2023, he celebrated 10 years since throat cancer.

Vaccines are now recommended for both females and males to prevent HPV-related cancers.
The Canadian National Advisory Committee on Immunization (NACI) recommends human papillomavirus (HPV) vaccination for females aged 9–26 years (bivalent or quadrivalent vaccine) and males aged 9–26 years (quadrivalent vaccine).
Hopefully, this awareness of vaccines will save much suffering and many lives in the future.
Barbara Carter Artist and writer with a focus on healing from childhood trauma, alcohol addiction, and living her best authentic life.
Likes to take walks, read, watch TV dramas, and practice Qi-gong, and work on her memoir series BARBARA By The BAY.





