

Infection | Brain
Largest Dataset Finds Prevalence of Covid-19 Neuropsychiatric Signs
It also adds on in that Covid-19 delirium was overlooked.
What the Largest Dataset Show
A group of neurology physicians and researchers in the US recently had their paper, “Spectrum of neuropsychiatric manifestations in COVID-19,” published in Brain, Behavior, and Immunity. They extracted data from the TriNetX Global Health Research Network — that compiles medical records from health care organizations across multiple countries — for Covid-19 records spanning January to July.
Their data analyses identified 40,469 confirmed cases of Covid-19, of which 9086 patients (22.5%) presented neuropsychiatric signs. More specific cohort details are as follows:
- Sex: Male (45%) vs female (55%).
- Age: 18–50 (48.7%) vs 51–80 (41.8%) vs >80 (9.5%) years.
- Residency: US (76%) vs non-US (24%).
- Race: Caucasian (37%) vs African American (21%) vs Asian (2%) vs unknown (40%).
- Settings: Outpatient (73.7%) vs inpatient (26.3%).
- Neuropsychiatric symptoms (22.5%): Anxiety (4.6%), mood disorders (3.8%), headache (3.7%), sleep disorders (3.4%), encephalopathy (2.3%), myalgia (2.0%), pain (1.8%), loss of taste and smell (1.2%), stroke and transient ischemic attack (1.0%), dizziness (0.9%), emotional disturbance (0.8%) extrapyramidal and movement disorders (0.7%), seizures (0.6%), polyneuropathy (0.6%), nerve root and plexus disorders (0.4%), and sucidal ideation (0.25).
These Covid-19 neuropsychiatric signs probably arise from a combination of, the authors wrote, “direct central nervous system infiltration, cytokine network dysregulation, peripheral immune cell transmigration, and post-infectious autoimmunity etc.” Mechanistic causation cannot be confirmed, owing to the study design that looks at the range and prevalence of Covid-19 neuropsychiatric symptoms. The strength is that the US TriNetX database study has the biggest sample size to date of 40,469 cases.

Comparison With Other Studies: Loss of Smell and Taste
Smell and taste are neurological rather than neuropsychiatric, as they involve nerves outside the brain. That said, the US database study found the prevalence of smell and taste to be at 1.2% only, which is very low. A June meta-analysis calculated it to be about 80%.
The researchers believe that it’s due to lack of its assessment in early times of the pandemic. Another reason is that loss of smell occurs more regularly in mild cases than hospitalized cases, as the destruction of olfactory neurons could be a defence mechanism to prevent virus invasion into the brain, as I detailed here:
Comparison With Other Studies: Confusion/Delirium
Data from smaller cohort studies, as summarized by a meta-analysis printed in The Lancet Psychiatry, also found that neuropsychiatric symptoms are typical in Covid-19 (see figure). But the meta-analysis mostly considers confusion (also called disturbed consciousness or delirium) only. The prevalence is much higher if headache, depression, anxiety, insomnia, or neurological diseases were included.
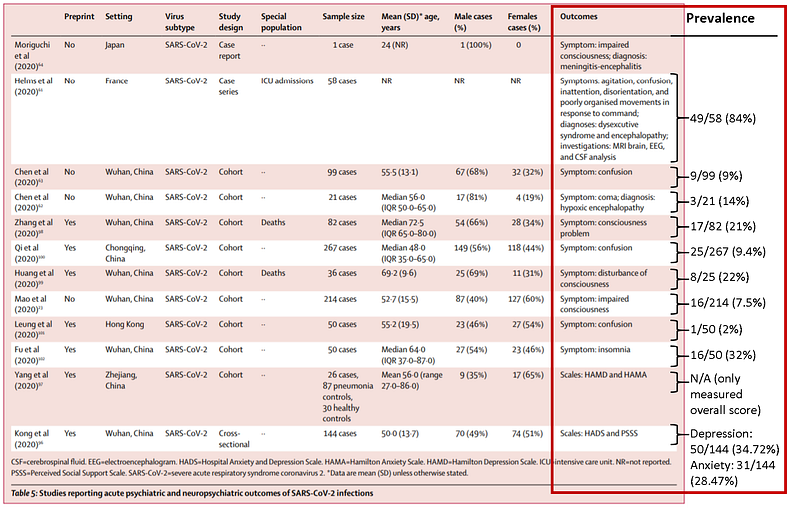
For example, the second-largest cohort study found that 36.4% of 214 patients had neurological signs, of which 24.8% involved the brain. In specifics, 16.8% had dizziness, 13.1% had headaches, 7.5% had disturbed consciousness, 2.8% had cerebrovascular diseases, 0.5% had ataxia, and 0.5% had a seizure. In the Lancet meta-analysis, however, only disturbed consciousness in this study was taken into account (see Mao et al. in the figure).
Based on the studies included in the Lancet meta-analysis, the frequency of confusion (or disturbed consciousness or delirium) is much higher than that of the US TriNetX database study. To reiterate, the US study found 0.9% and 0.8% of 40,469 Covid-19 patients had dizziness and emotional distress, respectively, which are signs of delirium.
The reason why the US database study did not measure delirium precisely is most likely because delirium was overlooked as a Covid-19 symptom until May, as I detailed here. Health professionals probably did not look for it and, thus, is missing in the TriNetX database. This is concerning as delirium is treatable and preventable, yet it is often disregarded. And survivors would then face life-long consequences of compromised brain health.



