Debunking ‘1 in 5 COVID-19 Patients Develop Mental Illness’
Alarmist press coverage is linked directly to a campaign in which authors exaggerate the clinical and public significance of their findings.

A media campaign orchestrated by the Science Media Centre of London spread a disturbing claim based on American electronic health records (EHRs) — that 1 in 5 COVID-19 patients would develop mental illness within 3 months of diagnosis.
Should we buy it?
We still have much to learn about the COVID-19 virus and its effects on the body and the mind.
There is a need to understand how we can best deploy scarce resources to deal with the long-term consequences of the virus and to rebuild health systems devastated by the pandemic.
We will see how misrepresentations of the significance of a study published in Lancet Psychiatry could lead to putting scarce mental health resources in the wrong places during the COVID-19 crisis and in its aftermath.
[Click here to tweet this quote.]
But we need to be careful. There is a lot of questionable information being put into peer-reviewed journals that are amplified by poor coverage in the media.
Should we worry about a mental health crisis and even a “tsunami of mental health problems” associated with COVID-19?
In this article, we will see how misrepresentations of the significance of a study published in Lancet Psychiatry could lead to putting scarce mental health resources in the wrong places during the COVID-19 crisis and in its aftermath.
The peer-reviewed article is available open access. If you like, read the article ahead of time or keep it open to check what I will be saying in this article. Complain on social media if you think I am misrepresenting the paper.
Taquet M, Luciano S, Geddes J, Harrison PJ. Bidirectional associations between COVID-19 and psychiatric disorder: retrospective cohort studies of 62,354 COVID-19 cases in the USA. Lancet Psychiatry.
Churnalism — What is it?
Newspapers and magazines around the world offered almost identical coverage of the article. The similarity is no accident.
Some sources cite the Reuters News Service, which provides stories to newspapers as a paid subscription service. However, many freelance journalists simply take credit for someone else’s work by attaching their name as the author in a byline.
This seems to have become an accepted form of plagiarism and has been given a special name, churnalism.
Churnalism is bad because it misleads with a false appearance of a spontaneous consensus among different sources. The nonprofit Sunlight Foundation has set up a free service to check for churnalism, just like teachers can check the papers students submit for plagiarism.
Hype in the Press Coverage
Euronews went to the trouble of interviewing one of the authors and here is the video:
Note also that Euronews had the independent judgment to label what was being discussed “mental health issues.
The Reuters coverage has direct quotes from a number of “independent” experts, creating the illusion that A journalist with Reuters conducted interviews.
Actually, I traced the direct quotes to a press release package created by Science Media Centre, London. We will dissect this “expertise” in my next article.
Welcome to the art of creating a buzz about a paper.
Many universities have paid staff whose responsibility is to keep count of authors’ mentions in media. Lots of mentions are good for bolstering the competitive advantage of the university brand versus its rival institutions. Needless to say, there is a lot of orchestration of press coverage, with forgettable “breakthrough discoveries” occurring all the time.
The Reuters headline that traveled around the world.
One in five COVID-19 patients develop mental illness within 90 days — study
Key snippets from Reuters
Many COVID-19 survivors are likely to be at greater risk of developing mental illness, psychiatrists said on Monday, after a large study found 20% of those infected with the coronavirus are diagnosed with a psychiatric disorder within 90 days.
“People have been worried that COVID-19 survivors will be at greater risk of mental health problems, and our findings … show this to be likely,” said Paul Harrison, a professor of psychiatry at Oxford.
[Professor Paul Harrison is senior (last) author on the Lancet Psychiatry paper]
Doctors and scientists around the world urgently need to investigate the causes and identify new treatments for mental illness after COVID-19, Harrison said.
“(Health) services need to be ready to provide care, especially since our results are likely to be underestimates (of the number of psychiatric patients),” he added.
There needs to be better availability of Personal Protection Equipment for clinicians, but probably not rubber rafts nor signs directing everyone to higher ground in the event of a tsunami of mental health problems.
[Click here to tweet this quote.]
Details from the Lancet Psychiatry article
This EHR network study used big data harvested from 69 million individuals enrolled in a US health care plan, 62,354 of whom had a diagnosis of COVID-19.
The authors determined whether having a diagnosis of COVID-19 was associated with increased rates of subsequent psychiatric diagnoses, as well as dementia and insomnia, being entered into the record from 14 to 90 days later.
The authors picked a specific time period (January-April 2020) to see whether having a new diagnosis of COVID-19 entered into the EHR was associated with a notation of a mental disorder 14 to 90 days later. They made comparisons with the mental health diagnosis noted for six groups of medical patients, those who received a diagnosis of:
· Influenza.
· Other respiratory tract infections.
· Skin infection.
· Cholelithiasis (gallstones).
· Urolithiasis (stones in the kidney, bladder, and/or urethra).
· Fracture of a large bone.
Taking advantage of such their large administrative data set, the authors selected patients in the six comparison groups by matching them for 50 variables — 28 variables reflecting risk factors for COVID-19 and 22 variables reflecting risk factors for more severe COVID-19 illness.
The authors found “survivors of COVID-19 appear to be at increased risk of psychiatric sequelae,” but the risk was unevenly distributed across diagnoses.
The likelihood of a diagnosis of a psychotic disorder after a COVID-19 diagnosis was low, about the same as for the other 6 physical health conditions.
New diagnoses of depression and other mood disorders (2%) were lower than for anxiety disorders. The results for depression are reassuring, but lower than what is typically found for medically ill populations when they are assessed with structured psychiatric interviews.
The most frequent psychiatric diagnosis after COVID-19 diagnosis was anxiety disorder (HRs 1·59–2·62, all p<0·0001), with a probability of outcome within 90 days of 4·7% (95% CI 4·2–5·3). Among anxiety disorders, adjustment disorder, generalised anxiety disorder, and, to a lesser extent, post-traumatic stress disorder and panic disorder were the most frequent.
And
The probability of a first diagnosis of insomnia was 1·9% (95% CI 1·6–2·2), which was more common than after control health events (HRs 1·85–3·29, all p<0·0001).
For dementia after a COVID-19 diagnosis:
The two to three times increased risk of dementia after COVID-19 infection extends findings from previous case series and is concerning.
But the authors seem to walk back the significance of that risk in the next sentence, as well as when the senior author was interviewed by Euronews. The Lancet Psychiatry article said:
Some of the excess might reflect misdiagnosed cases of delirium, or transient cognitive impairments due to reversible cerebral events.
The authors are thus questioning the reliability of a diagnosis of delirium (Would it change over time?) and even its validity (Could it be a “misdiagnosis”?).
I will take this as a cue for a more general critique of the recordings of diagnosis in this study and the implications that are for how to deal with the COVID-19 crisis and its aftermath.
We don’t need an army of mental health clinicians mobilized to deal with COVID patients’ problems in adjusting to their illness and the other disruptions the pandemic brings to their lives. A little support, encouragement, and practical assistance would go a long way, even if providing this is not a billable procedure.
Critique
The study is huge by any standards, but the diagnoses noted in electronic records are unlikely to be clinically and scientifically valid with any precision.
The clinicians entering data into medical records are on the frontlines during a terrible health care crisis. They are primary care and specialty care, but not typically from specialty mental health care. They do not have much formal training in making mental health diagnoses. Nor do they relying on a structured interview guided by formal diagnostic criteria.
The clinicians are making diagnoses mainly for administrative purposes, justifying procedures or prescriptions or time spent with patients.
Many medical settings in the US have EHR depression/mental health screening and follow up platforms. Clinicians cannot close an EHR and go on to their next patient without clicking “yes” to the prompt, “Did you inquire about mental health?” A positive response to a crude screening question from the patients requires that the clinician ask further questions and indicate what action was taken.
I have supervised studies with thousands of primary care, psychiatric, and general and specialty medical patients. A structured interview typically takes 30 to 90 minutes, depending on how many symptoms patients endorse and what probing or explaining of symptoms the interviewer has to do.
For instance, someone with a fractured leg might endorse “little interest or pleasure in doing things.” However, the interviewer inquiring further about this will quickly discover that the patient is referring to not being able to dance, do Pilates, or walk the dog. What is not meant is a loss of the ability to experience pleasure, which is a defining symptom of depression, anhedonia.
So, let’s look at the increase in the recording of anxiety disorders, which drove the authors’ conclusions.
A formal diagnosis of a general anxiety disorder (GAD) requires a duration of six months, but clinicians will often endorse GAD based on the patient being anxious or worried in a single medical encounter. I strongly suspect that a typical diagnosis entered for GAD would not be met the criteria for duration or number and severity of symptoms
Patients with COVID-19 frequently report breathing difficulties, which can be frightening, and they may even hyperventilate. But mostly these symptoms can be managed as pulmonary, not mental health problems.
A formal diagnosis of PTSD requires a precipitating event and endorsement of symptoms that overlap with symptoms that would otherwise contribute to a diagnosis of depression. I doubt many of these patients would be diagnosed as having PTSD if formally interviewed by a trained mental health professional. Rates were low, anyway.
Finally, there is an increase of the diagnosis of adjustment disorder.
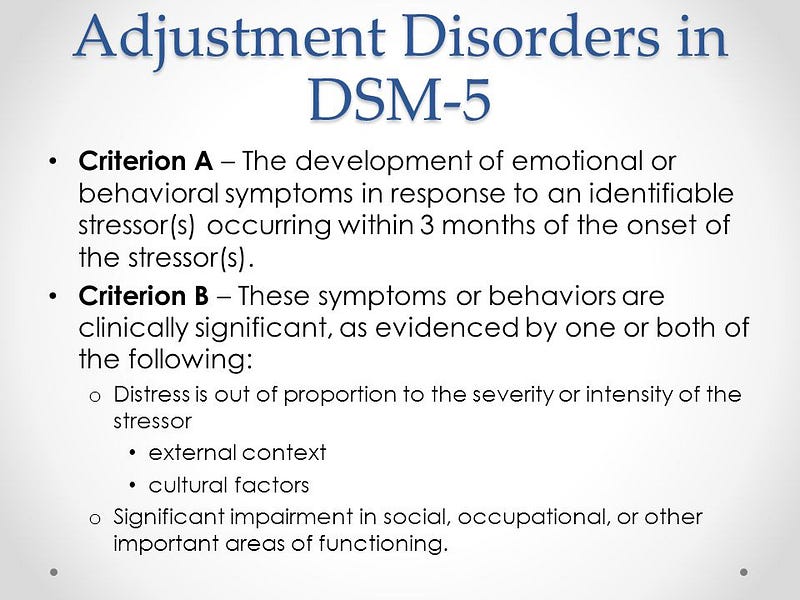
This diagnosis is only applied to patients who do not meet the criteria for other diagnoses. Major depression, psychosis, and panic, and general anxiety disorder have to be ruled out. As can be seen in the box from Mayo Clinic, a diagnosis would be warranted by the patient experiencing understandable distress after contracting COVID.
An accurate, non-alarmist interpretation of these results is that after a COVID-19, there is little increase in depression, little or no increase in severe mental disorder, but patients more commonly report being anxious.
[Click here to tweet this quote.]
A diagnosis of adjustment disorder would not fit with intelligent lay ideas about mental illness.
Some of us who supervise diagnostic mental health interviews for scientific purposes jokingly refer to an adjustment disorder as an “acute compensation reaction” on the part of clinicians who need to justify reimbursement for their services.
[Click here to tweet this quote.]
Most patients who answer “yes” to the mental health screening question because they are sad or worried, but did not fit depression or an anxiety disorder. Unless clinicians enter a mental health diagnosis, they may not close the patient's medical record, get paid, or justify not doing something else. Some settings penalize clinicians for not adhering to these rules.
Administrative diagnostic data, unless dramatically different than what these authors abstracted from EHRs, does not justify calling a press conference with serious pronouncements about mobilizing a clinical and public health response.
An accurate, non-alarmist interpretation of these results is that after a COVID-19, there is little increase in depression, little or no increase in severe mental disorder, but patients more commonly report being anxious.
The data are not great scientifically, but within this limitation, the data do not signal a mental health crisis.
The impact of COVID-19 on the health care system is huge. The virus places a huge strain on the general medical system, depletes resources, and causes infection and deaths of frontline clinicians and support workers. There is a disruption of face-to-face mental health care, the closing of halfway houses and aftercare, loss of inpatient psychiatric beds, and patients being unwilling or unable to leave their homes for outpatient visits.
We need to address the unmet need for services and social disparities in health care that predated COVID-19. We need to be prepared for a modest increase in mental health problems, particularly among persons who are otherwise vulnerable and disadvantaged.
There needs to be better availability of Personal Protection Equipment for clinicians, but probably not rubber rafts nor signs directing everyone to higher ground in the event of a tsunami of mental health problems.
But, for Pete’s sake, we don’t need an army of mental health clinicians mobilized to deal with COVID patients’ problems in adjusting to their illness and the other disruptions the pandemic brings to their lives. A little support, encouragement, and practical assistance would go a long way, even if providing it is not a billable procedure.
If you like this story, follow me on Medium, Twitter, or Facebook.