
Could this be the Next Best Method for Prenatal Screening?
Single Nucleotide Polymorphisms are being detected in non-invasive prenatal tests to predict inheritance of fetal abnormalities.
Prenatal screening tests can identify if a fetus is predisposed to certain birth defects that are usually genetic. Some of these screenings include serial detection of maternal serum, ultrasound, amniocentesis, and chorionic villus sampling (CVS). Serial detection of maternal serum coupled with nuchal translucency as well as cystic hygroma indicators on ultrasound are often associated with false-negative rates from 12% to 23%. Additionally, detection rates range from only 75% to 96% (depending on the screening approach utilized) and are accompanied by false-positive rates ranging from 1.9% to 5.2%. Confirmatory invasive methods such as amniocentesis and CVS require needle insertion through the skin and into the uterus to collect the samples needed leading to risk of infection, bleeding, or miscarriage.
Non-invasive prenatal testing (NIPT) using cell-free fetal DNA (cffDNA) floating freely in maternal plasma, was introduced clinically in 2011 as a screening method for trisomy 21 (Down syndrome). This NIPT has been well accepted by clinicians as a test for women with increased risk of fetal aneuploidy and it has now been extended to low-risk women in privatized settings4. cffDNA is derived from the syncytiotrophoblast layer of the placenta circulating freely in the maternal blood5. It has revolutionized our ability to screen for common aneuploidies in the fetus such as trisomy 21, trisomy 18 (Edwards syndrome), and trisomy 13 (Patau syndrome). cffDNA screening may also identify fetal sex, fetal sex chromosome aneuploidies, and more recently microdeletions and monogenic disorders.
The deployment of Next Generation Sequencing (NGS) to study whole genome and targeted sequences has enabled the widespread adoption of the use of NIPT as a first-tier test in clinical settings. This test provides an accurate measure of fetal fraction which is a measure of the amount of cffDNA relative to the total amount of circulating cell-free DNA (cfDNA) in maternal plasma. It is also a determinant of assay sensitivity, with an average fetal fraction range of 10–15% between 10 and 20 weeks of gestation5. Previously, Y chromosome specific markers were used to quantify fetal fraction however, the use of SNP ratios estimates fetal fraction regardless of the fetus’ sex.
The first SNP-based NIPT method used allele specific PCR amplification of SNP markers from paternal and maternal buffy coats and cfDNA in maternal plasma. Comparison of the maternal plus fetal bands with the unique fetal band intensity allowed estimation of the fetal chromosome 21 dosage while unique paternal SNPs were used to estimate fetal fraction. Current SNP-based technology is a targeted qualitative method using multiplex PCR of highly polymorphic SNPs followed by NGS to assess the variation of single nucleotides in the DNA sequence and copy number variations.
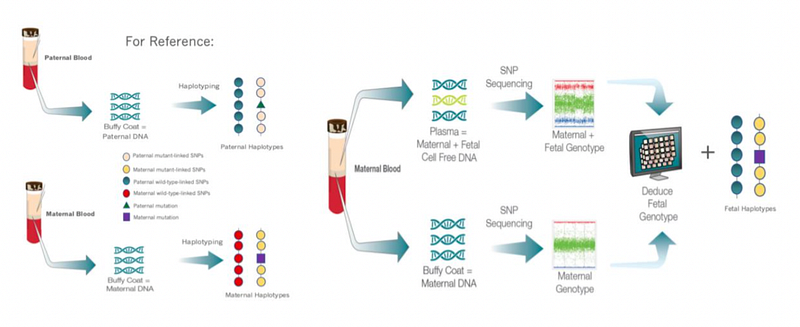
Figure 1. SNP-based Non-Invasive Screening Methods for Monogenic Diseases, Aneuploidies, and Microdeletions. The left side indicates collection of paternal and maternal DNA sources for sequencing and phasing into haplotypes which will later be used as references to determine fetal inheritance of the haplotypes. Circles denote polymorphic alleles, triangle represents the paternal mutation, and square represents the maternal mutation. On the right side after pcr amplification and sequencing an algorithm deduces fetal genotype through the sum of the contribution of both maternal and fetal allele reads as a function of fetal fraction. A risk score is determined for each chromosome or microdeletion site by comparing maximum likelihood information of the SNPs to actual sequencing information. At the far-right side we can see the result of fetal inheritance from sequencing reads that were aligned and analyzed by relative haplotype dosage (RHDO) with the reference of parental haplotypes.
A limitation of the SNP-based NIPT is that it cannot be offered to patients who are surrogates or have received an egg-donation from an unrelated donor. Additionally, the SNP-based method relies on heterozygous sites in the mother to detect aneuploidy of maternal origin. The data becomes uninformative in cases with high levels of homozygosity between mother and fetus, possibly due to consanguinity or segmental uniparental disomy.
The availability of a fast-reproducible test with no invasive risk to the fetus makes NIPT a highly recommended choice for all pregnancies. The detection of separate fetal and maternal DNA makes the SNP-based approach a powerful choice in clinical settings, not just for detection of common aneuploidies, but also for screening of microdeletions. Moreover, SNP-based NIPT opens the door to being a cost-effective, relatively low-resource screening technique for evaluation of other pediatric diseases such as beta-thalassemia and cystic fibrosis, by allowing detection of source alleles including alleles of paternal origin. Emerging, is the possibility for design of more unique sets of primers to target other known disease informative SNP loci. The major drawback of this technique is the high rate of false positives and “no-calls” due to low fetal fraction. Reflex sequencing with higher read depths for “high-risk” calls as well as modified risk scores for trisomy 13 and 18 can mitigate this issue. Novel methods offer improvements for the sensitivity of the test by leveraging chromosomal phase information to lower the threshold for minimum fetal fraction. The constant expansion and improvement in prenatal screening of informative SNPs minimizes the number of women who need to get unnecessary invasive testing and the number of affected pregnancies that go undetected.





