
Back in the Spotlight: Hydroxychloroquine for COVID-19
Retrospective study shows a benefit to hydroxychloroquine if given early and lower dose than used in RECOVERY Trial
The data on whether hydroxychloroquine benefits patients with COVID-19 are inconsistent. Some early studies with very small numbers of patients showed benefit in reducing viral load. Initially, the World Health Organization (WHO) included hydroxychloroquine as one of the 4 treatments in the SOLIDARITY Trial for patients hospitalized with COVID-19 but has since stopped this arm of the trial. The NIH stopped a clinical trial of hydroxychloroquine for hospitalized COVID-19 patients.
The WHO notes in their decision that the decision to stop this arm of the SOLIDARITY Trial does not mean that hydroxychloroquine (or the other arm testing another treatment that was discontinued) are not potentially useful in patients with mild symptoms or as potential preventative therapy:
“…does not affect the possible evaluation in other studies of hydroxychloroquine or lopinavir/ritonavir in non-hospitalized patients or as pre- or post-exposure prophylaxis for COVID-19.”
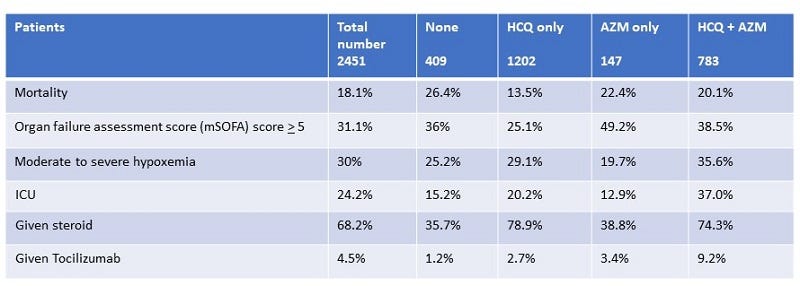
In light of this comment from the WHO, a retrospective study that evaluated the medical records for 2,541 COVID-19 patients in a 6 hospital medical system in Detroit, Michigan. They compared the mortality of patients who received hydroxychloroquine, hydroxychloroquine + azithromycin, azithromycin, or none of these treatments. As with most of the COVID-19 treatment studies, there were many variables ranging from different ages to body mass index and other disease conditions, such as chronic lung disease or cardiovascular disease. Additionally, other treatments, such as whether the patients received corticosteroids or tocilizumab, varied. Thus, the data are complicated with many confounders that make it difficult to assess whether any differences in mortality related to the use of hydroxychloroquine or azithromycin.
Despite this complexity, the researchers found statistically meaningful information from this set of patients.
Predictors of mortality, regardless of treatment, included
- age greater than or equal to 65 years
- chronic kidney disease
- low oxygen saturation upon admission
- need for artificial ventilation during admission
- white (race)
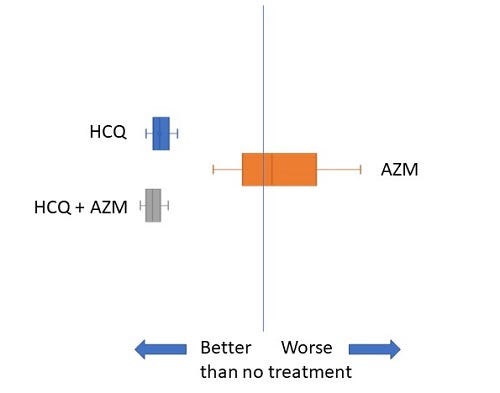
Hydroxychloroquine with or without azithromycin reduced the risk of death.
These results should be interpreted cautiously. In the subset of characteristics noted above, two seem particularly important. Many more of the hydroxychloroquine-only patients also received steroids, which have now been shown to benefit COVID-19 patients in a clinical trial (Horby et al.). Additionally, this group of patients also had a lower proportion with higher scores of modified organ failure assessment. Higher scores are associated with worse outcome. So, the patients in the hydroxychloroquine-only group could have been less sick than the other groups.
Because the patients were so diverse, the researchers also took a subset of the patients that had the similar characteristics in 18 of the variables. There were 190 that received hydroxychloroquine and 190 did not. This part of the study is particularly important because it reduces the effects of these variables. However, this part of the study could have too few patients in each group to provide truly useful information, and azithromycin treatment was a variable in both groups. Some of the 190 in each group received azithromycin. However, this can help address whether the difference related to the higher use of steroids and the relatively lower severity (based on modified sequential organ failure assessment) of disease in the full set of patients receiving hydroxychloroquine.
With this matched set of patients, hydroxychloroquine provided a survival advantage using 2 different assessment methods. Cox regression analysis predicted a reduction in mortality by ~50%, compared to those not receiving hydroxchloroquine. The patients who received hydroxychloroquine had a ~90% survival probability 28 days after admission. In contrast, those not receiving hydroxychloroquine had ~80% survival probability 28 days after admission.
This retrospective study found different results from another retrospective study of US veterans hospitalized with COVID-19 by Magagnoli et al. and an observational study by Geleris et al. Their results also differ from those of randomized clinical trials, such as the hydroxychloroquine arm of the RECOVERY Trial.
When asked how they explain these differences, Dr. Marcus Zervos, a co-author on the study, said
“ We attribute our findings that differ from other studies to early treatment… Our dosing also differed from other studies not showing a benefit of the drug.”
The SOLIDARITY Trial and RECOVERY Trial used higher doses of hydroxychloroquine. Many of the other studies examined patients who were much sicker than those in this retrospective study.
Unfortunately, there is so much variability across the patients and trial protocols, it is hard to compare the results of all of the studies. Thus, this latest report supports keeping hydroxychloroquine in the treatment options, at least for early stage patients with relatively mild symptoms.
Highlighted Article
Arshad, et al., Treatment with Hydroxychloroquine, Azithromycin, and Combination in Patients Hospitalized with COVID-19. International Journal of Infectious Diseases (01 July 2020) DOI: https://doi.org/10.1016/j.ijid.2020.06.099
Related Reading





