
As a Physician, I Want You to Stop Your Medications
Patients and doctors should share the decision-making process to lessen dependence on drugs

“Mrs. Jones, I see you are here today for headaches and high blood pressure. Your pressures are very elevated. Have you been taking your blood pressure medication?”
“I do… but not every day.”
This sort of exchange would always frustrate me, as the reasons for coming to see me are so preventable. The ER is completely flooded and here is a patient who could have stayed home by just taking medications as prescribed.
Recently, as I’ve stepped away from my daily grind in the ER and taken a broader view, I’ve realized that these issues can be systemic, even though they appear individual. What are the barriers for this patient taking her medications? If she has a perfect understanding of the medication and her condition, then her lack of using the medicine is her fault. However, often the information flow to the patient is not perfect or even complete. Patients have to trust their doctors. However, with time constraints created by the medical system, the personal relationship with doctors has been tarnished.
As physicians are the forward-facing part of the profit-first medical business, it is assumed that they benefit from prescribing medications. Coupled with cost barriers, patient trust decreases and they are less likely to adhere to medications. However, physicians do not benefit from prescribing and they want their patients to be off of medications.
Why many prescribed medications are not taken
About 1 in 5 U.S. prescriptions go unfilled, it turns out. I had no idea this was the case, even after years of working in medicine. My thinking was that I wrote a prescription and a patient went to get it right after our visit together. But this just is not the case.
About three in ten of all adults report not taking their medicines as prescribed at some point in the past year because of the cost. This includes about 20% who say they didn’t fill a prescription or took an over-the-counter drug instead. About one in 10 patients say they cut pills in half or skipped doses.
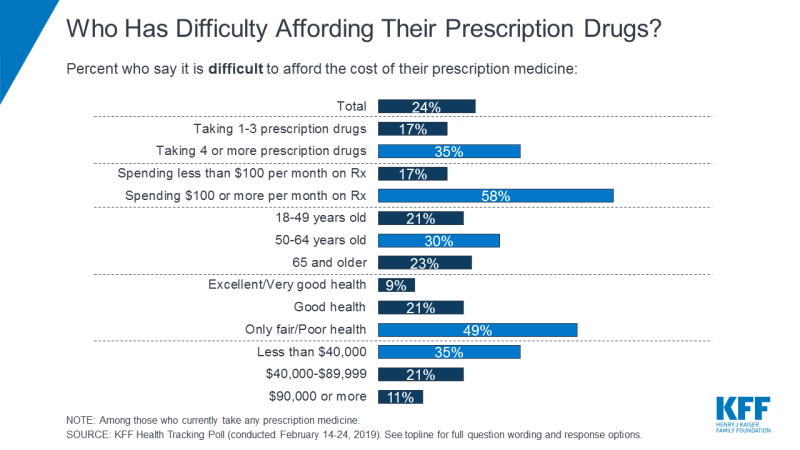
Many people have issues with affordability. As seen in the chart below from the Kaiser Family Foundation, this directly correlates with age (up to 65) and the number of medications. The sicker you are, the harder it is to obtain your medications. Same goes if you are poor.
The problem is that sick people often need more medications, especially as chronic conditions worsen. Barriers like cost and access to care make these conditions worse as they are left untreated. However, under all circumstances, it is my job to make a patient understand why a certain medication is recommended. That starts with trust.
Shared decisions help with adherence
Shared decision-making, first coined in 1982, is a process whereby clinicians collaborate with patients to reach well-informed medical decisions. This process is especially relevant in conditions where there is a close trade-off between harms and benefits. As a physician, I offer the evidence behind my thought process but I leave it up to the patient. Patients should lead the discussion toward what matters most to them when it comes to health, life, and financial decisions.
Often I will hear, “You are the doctor, you decide.” Patients are right to think this way. They have insurance so they came to see the expert.
So why am I asking them for their opinion? Because health is a relationship with your body. I am here to offer the advice I know. I cannot make decisions for what you will or will not do for your health. That will come from education mostly and all I can do is teach what I know.
I try to put myself in the shoes of my patients whenever I can. Empathy builds trust. But I also believe strongly in patient autonomy and want them to understand their medical issues. I can share only what I know and try to be humble enough to tell patients when I do not know something. I think shared honesty is just as important as shared decision-making. If a patient is going to be vulnerable with me at very important moments in their life, I have to earn their trust with honesty. This is the only way I can help a patient get to a healthy state.
Many medications are expected to be used by a patient for the rest of their life. It is condition dependent since the severity of a disease process will dictate dose, medication type and the possibility of stopping the medicine in the future. Diabetes can be reversed if you still produce insulin. Hypertension can be reversed with sustained weight loss and diet change. Arthritis can be mitigated with physical therapy so less medications are needed. We are lucky to live in an age where medications are widely available; as long as we use them only when needed.
Coming up with a plan together for the future
Once a patient and I have decided to start a medication, it is important to establish future expectations. For example, diabetes should be tracked every three months. High cholesterol levels are tracked every six months to a year. Each condition has its own follow-up schedule.
Adherence to medications will either depend on physical results (fewer headaches with controlled blood pressure) or simply based on trust from the established relationship with a physician.
Ultimately, a medicine should only be continued if it is helping. This can mean some specific measurement gets better (like the glucose in your bloodstream if you are diabetic) but more importantly it means improved quality of life, reduced symptoms, and feeling better. I always tell patients that lab values are necessary to guide decisions, but how you feel day-to-day is so much more important.
By using shared decision-making and trusting their physician, medications can be of great value to help patients. If I think starting a medication will improve someone’s quality of life, I will recommend it. I will then do everything in my power to help get my patient off of that medication. I believe this approach gives my patients the best chances for a healthy, long life.





