
SCIENCE
Analysis of Musician’s Dystonia: Part I
Unveiling complex musical injury

Introduction
Robert Schumann, born in Zwickau, Saxony in 1810, was a major composer and highly skilled pianist of the early romantic period. While developing his performance career, extensive diary entries described that his progress was interrupted by loss of control in his right hand’s middle finger. After unsuccessful interventions including use of a contraption designed for finger stretching, homeopathy, and soaking his hand in animal blood, he stopped playing piano repertoire and was limited to improvising.¹
Schumann suffered from a neuromuscular disorder known as Musician’s Dystonia, an injury that interferes with the careers of 1% of professional musicians it strikes. Generally, most have solo positions with monstrous workloads, anxiety with perfectionist tendencies, and a family history with MD.² ³ Statistical data, including a retrospective study of 144 musicians with MD suggests a proportion of male to female sufferers as 4:1, with pianists, guitarists, and brass instrumentalists at highest risk of developing symptoms.⁴⁵
“Musician’s Dystonia presents itself as a painless muscular incoordination or loss of voluntary motor control of extensively trained movements while a musician is playing the instrument.¹ ”
How it Manifests
There is a link between specific fingers and hands with the highest workload, and the onset of symptoms. In keyboard and non bowing string instruments most affected digits are three, four, and five of the right hand, and bowing string instrumentalists are mostly affected in digits three through five of the left.⁶ ⁷
MD is task specific because it manifests while playing the specific instrument that triggered it.⁸ The first symptoms include a subtle loss of control in fast passages, later developing into involuntary curling or flexing of fingers, and loss of the mouth-to-instrument control (aka embouchure) in wind instrumentalists.⁵ Although pain is not usually associated with MD, muscular strain can result from secondary symptoms, which are co contractions of different muscle groups in attempts to compensate for faulty movements.⁷
Making Sense of Mystery
The cause and nature of MD is not entirely understood, so it is described as an idiopathic illness.⁹ Although, studies of MD reveal abnormalities in inhibitory systems in the brain/central nervous system, the basal ganglia, and maladaptive plasticity as observed in studies using magnetoencephalography (MEG), MRI, and transcranial magnetic stimulation (TMS).¹⁰ ⁴ ¹¹ ¹²
“Maladaptive plasticity refers to the plasticity in the nervous system that leads to a disruption of the function and may be considered as a disease state.¹³ ”
Trigger Factors
Jabusch and Altenmuller (2006) explain that predisposing factors of male gender, and family history of MD may interact with other factors, resulting in a triggering of MD symptoms.
Intrinsic trigger factors
These include physical disorders like trauma and overuse injury. Compression, especially of the ulnar nerve has been theorized as another factor in that it interacts with muscles controlling digits 4 and 5.¹⁴ As mentioned before, preexisting psychological traits like trends toward perfectionism and anxiety have often been displayed by sufferers.²
Extrinsic trigger factors
These lie in the genre of classical music, where special temporal sensorimotor constraints, alongside extreme musical and social pressures are prominent, making more sufferers classical musicians.⁶ ⁷ ¹⁵ This is reinforced by Berque, Gray, Harkness, and McFayden (2010, pg. 149) , where they mention that:
“Musician’s Dystonia is thought to be related to the intense and prolonged practice of rapid, alternating, and highly precise finger movement patterns.¹⁶ ”
Origins of Faulty Brain Wiring
Primate model
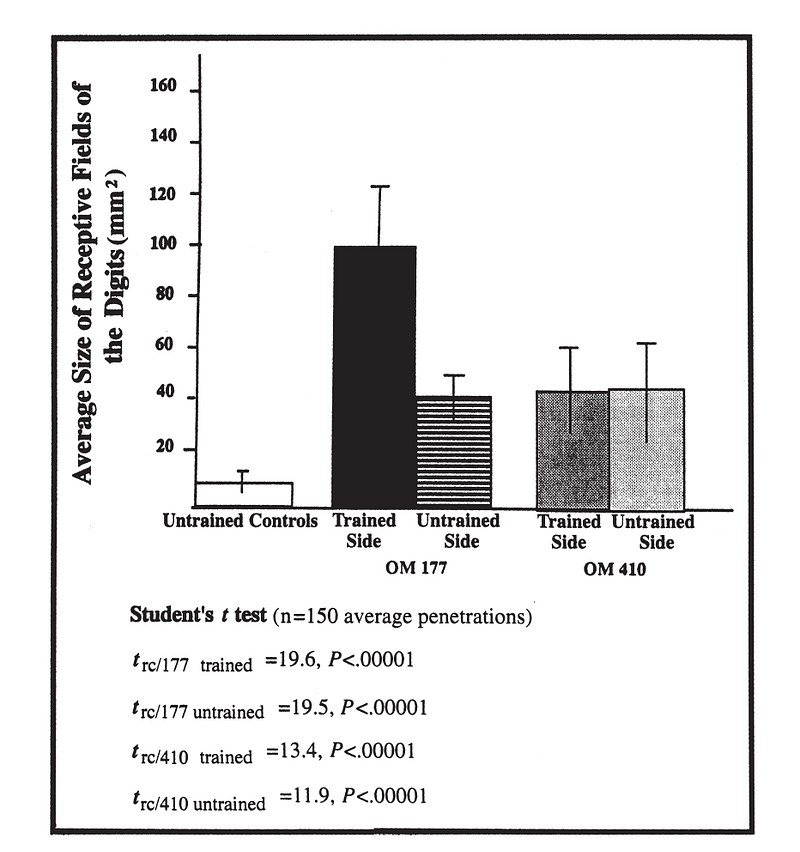
As I covered earlier, the pathophysiology of MD is still unclear, but a prominent model is based on maladapive plasticity. It is seen in dedifferentiation of neural networks responsible for the representation of the hand through repetitive use. Think of this as tangled brain wiring.¹⁷ This was first observed by by Byl, Merzenich, and Jenkins (1996) in monkeys who performed daily repetitive hand movements, including opening and closing the hand, and spreading the thumb and index finger apart to pinpoint targets.¹⁸
Several of the monkeys who completed the pointing task developed classic symptoms of focal dystonia, and a degradation of the somatosensory cortex was observed with enlarged receptor fields. These are sensory receptors that activate corresponding muscles. See figure 1 below. A substantial overlap of representations of the first and second fingers was seen using an electrode which mapped the cortex during daily exercises.
Human model
Similarly, human participants with focal dystonia exhibited degraded finger representations in the somatosensory cortex when compared with healthy participants.¹⁹ In Elbert, Candia, and Altenmuller (1998), (MRI) and (MEG) testing revealed fusions of the cortical representations of affected digits in the primary somatosensory cortex of eight musicians affected with MD compared to non-dystonic musicians and controls.
Conclusion
These models point to neurological mechanisms contributing to a complex injury that can severely impact the quality of life of some musicians. Therefore, it is vital to present treatment plans rooted in existing research. Byl and Priori (2006) state that based on the hypothesis of defective learning expressed by neural maladaptation observed in MD sufferers, effective behavioral treatment could reverse degradation to the central nervous system that may be responsible for symptoms to begin with. Based on this hypothesis I will reveal multiple behavioral treatment interventions available, and include a notable case study in the Part II of this series.
References
- Jabusch, H.-C., & Altenmüller, E. (2006). Focal dystonia in musicians: From phenomenology to therapy. Advances in Cognitive Psychology, 2(2–3), 207–220. https://doi.org/10.2478/v10053-008-0056-6
- Jabusch, H.-C., Müller, S. V., & Altenmüller, E. (2004). Anxiety in musicians with focal dystonia and those with chronic pain. Movement Disorders, 19(10), 1169–1175.
- Schmidt, A., Jabusch, H. C., Altenmüller, E., Moeller, J., Goebel, A., Kasten, M., & Klein, C. (2012).Challenges of making music: An environmental case-control study of musician’s dystonia. In MOVEMENT DISORDERS (Vol. 27, pp. S363–S363). WILEY-BLACKWELL 111 RIVER ST,HOBOKEN 07030–5774, NJ USA.
- Lim, V. K., Altenmüller, E., & Bradshaw, J. L. (2001). Focal dystonia: current theories. Human Movement Science, 20(6), 875–914.
- Ioannou, C. I., & Altenmüller, E. (2014). Psychological characteristics in musician׳ s dystonia: A new diagnostic classification. Neuropsychologia, 61, 80–88.
- Tubiana, R., & Chamagne, P. (2000). Prolonged rehabilitation treatment of musician’s focal dystonia. Medical Problems of the Instrumentalist Musician. London: Martin Dunitz, 369–378.
- Brandfonbrener, A. G., & Robson, C. (2004). Review of 113 musicians with focal dystonia seen between 1985 and 2002 at a clinic for performing artists. Advances in Neurology, 94, 255–256.
- Altenmüller, E. (2003). Focal dystonia: advances in brain imaging and understanding of fine motor control in musicians. Hand Clinics, 19(3), 523–538.
- Watson, A. H. D. (2009). The Biology of Musical Performance and Performance-Related Injury (Pap/Cdr edition). Lanham, Md: Scarecrow Press.
- Elbert, T., Candia, V., Altenmüller, E., Rau, H., Sterr, A., Rockstroh, B., … Taub, E. (1998). Alteration of digital representations in somatosensory cortex in focal hand dystonia. Neuroreport, 9(16), 3571–3575.
- Altenmüller, E., & Jabusch, H.-C. (2010). Focal Dystonia in Musicians. Med Probl Perform Art, 3–9.
- Rosenkranz, K., Altenmüller, E., Siggelkow, S., & Dengler, R. (2000). Alteration of sensorimotor integration in musician’s cramp: impaired focusing of proprioception. Clinical Neurophysiology, 111(11), 2040–2045.
- Li, Xiang-Yao et al. “Maladaptive Plasticity and Neuropathic Pain.” Neural plasticity vol. 2016 (2016): 4842159. doi:10.1155/2016/4842159
- Charness, M. E., Ross, M. H., & Shefner, J. M. (1996). Ulnar neuropathy and dystonic flexion of the fourth and fifth digits: clinical correlation in musicians. Muscle & Nerve, 19(4), 431–437.
- Schuele, Stephan U., and Richard J. Lederman. “Occupational disorders in instrumental musicians.” Medical Problems of Performing Artists 19.3 (2004): 123–128.
- Berque, Patrice et al. “A combination of constraint-induced therapy and motor control retraining in the treatment of focal hand dystonia in musicians.” Medical problems of performing artists vol. 25,4 (2010): 149–61.
- Byl, N. N., & Priori, A. (2006). The development of focal dystonia in musicians as a consequence of maladaptive plasticity: implications for intervention. Music, Motor Control and the Brain Edited by and Eckart Altenmüller, Mario Wiesendanger and Jürg Kesselring, 293–308.
- Byl, N. N., Merzenich, M. M., & Jenkins, W. M. (1996). A primate genesis model of focal dystonia and repetitive strain injury I. Learning-induced dedifferentiation of the representation of the hand in the primary somatosensory cortex in adult monkeys. Neurology, 47(2), 508–520.
- Leighton B.N. Hinkley, Rebecca L. Webster, Nancy N. Byl, Srikantan S. Nagarajan. Neuroimaging Characteristics of Patients with Focal Hand Dystonia, Journal of Hand Therapy,Volume 22, Issue 2, 2009.





