
Americans Are Still Dying of Opioid Overdoses
Why won’t we do something about it?
A dust cloud is covering the southeast. The number of coronavirus cases in the United States is now daily at 40,000 and rising in this COVID-19 pandemic. People are filling up hospitals. George Floyd marches and others are still going on yet, BIPOC are being arrested for jaywalking and dancing in the street.
The European Union (EU) agrees to reopen borders to 14 countries, and is extending a travel ban for US tourists. Extending? It sounds like the EU is doing us a favor, but I can assure you that they are not. It’s like they didn’t want to simply say that Americans are banned from the EU.
But in the background, our culture is being killed by opioid abuse. Americans are still dying. The coronavirus is a pandemic, yes. But the opioid crisis is an epidemic that never stops. What’s the difference? A pandemic is a disease that covers a wide plethora of countries. An epidemic is limited to a community.
Our American community is plagued by continuous opioid deaths.
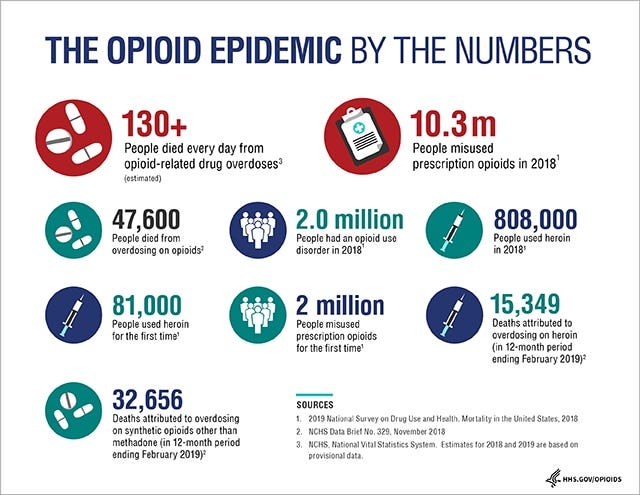
We’re losing 130 Americans a day to opioids. It’s maddening to think about what is happening to our mortality rate. Between the coronavirus, the coming flu season, and the opioid crisis, we are losing control.
We don’t have to kill Americans.
Psychologically we don’t have the will to stop murdering our citizens. Over the last fifty years, we have purposely stopped any innovative approaches that would help them live longer…opting instead to punish them by criminalizing drug abuse. Something about it must make somebody feel better inside.
We called drug dealers “pushers” in the 1970’s TV shows. Starsky and Hutch busted them in the imaginary Bay City, California running the streets in a Ford Gran Torino. Maybe it was my imagination, but their “police” characters had a whiff of illegality about them like they wouldn’t be above planting drugs on those they didn’t like — just to get them off of the street. If one ever stopped to notice, the drug trafficking never ever stopped. The drugs kept on coming. But we never seem to learn.
Like poverty and taxes, drugs will always be with us.
First Lady Nancy Reagan made a grand effort to help in the “War on Drugs” in the 1980s. Her slogan was “Just Say No.” She traveled the country and other countries — at least 250,000 miles of travel, in order to spread the word.
But I also remember this — jokes were made about the inefficacy of the message. And what if you didn’t say no? Did that mean you were bad? Second-class? A throwaway?
She said if she could save one person, it was worth it. With that standard, she may have been successful. I’d like to think she saved thousands.
Like poverty and taxes, drugs will always be with us.
We‘re going to have to walk and chew gum at the same time.
The coronavirus is deadly. The flu can be; according to the science and medical experts, we’re gearing up for a heavy season. Complicating the issue is the fact that one can have the coronavirus and the flu at the same time because contrary to some beliefs, these are two very separate diseases.
“Globally, about 3.4% of reported COVID-19 cases have died. By comparison, seasonal flu generally kills far fewer than 1% of those infected.”
And we have the opioid crisis. We have to somehow, with our nation of 330 million, attack all three killers at the same time. We’ve got the expertise and the knowledge.
All we lack is the will.
We can go back to treating opioid use as an illness and not a personal flaw.
In the 1800s, drug use was considered a public health problem. But in the early 1900s, prohibition became the goal. Narcotic clinics, used to help monitor the usage of addicts, thereby helping them stay away from illegal means and live longer, were shut down. Even though whites used drugs even more than the black community then and now, it was instead used to criminalize minorities in a racial twist:
“Politicians, pastors, and the press drew specious links between drug abuse and the exploitation of white women.”
But the fact was:
“Indeed, historian David Courtwright concludes that “southern whites [of the era] had the highest addiction rate of any regional racial group in the country and perhaps one of the highest in the world.”
The era in question that David Courtwright wrote about is the years between 1860 to 1920.
Even the New York Times was on the bandwagon:
“*Some newspapers later claimed cocaine use caused blacks to rape white women and was improving their pistol marksmanship.”
Cocaine helps Blacks shoot their pistols with more accuracy!?
(Shush! Don’t tell anyone!)
When America switched from treating drug addiction as a health problem to one of criminality, we set the stage for the creation of an underclass.
We also set the stage for death.
There has been a change in recent years.
As the opioid devil took the White community under its wing, there has been a change in attitude. Putting Black addicts into prison and throwing away the key was not an option for their White peers. All of a sudden, “forgiveness” programs were created.
“White America has opened its eyes to the evils of the drug war at the very moment that the opioid epidemic has begun to plague rural and predominantly white communities.”
It’s ironic, though. The racist emphasis on black opioid criminality led to some painful hours. When I had dental surgery, I was told to take Tylenol from the grocery store.
There is a false belief that Black people don’t feel pain like White people. This has impacted the medical treatment of millions of my Black brothers and sisters. The fear was so great that we’d become addicted, so out of love I suppose, we were left to live and work in pain. It had nothing to do with the availability of medical coverage — I’ve had that for all of my life. This is a racial bias, born out of racism.
This was taken from a report about the biases of medical trainees in the Association of American Medical Colleges (AAMC). This document is dated not 1920, but January 6, 2020.
Remember my comment about Tylenol?
My White friend’s seventeen-year-old son had dental surgery — nowhere near as involved as mine, and was given a bottle of 30 oxycodone pills. Overkill, much? That smart woman replaced the pills with Tylenol. He took two and was done.
She was not going to take a risk.
In another situation, a young White “recovering” drug addict, who is a close family friend, just had a baby.
She was honest about her drug problem with the medical staff and still received a bottle of 30 hydrocodone pills when she was released. She took five of them all at once…yesterday. I’m in another state. I can’t do anything about it.
White people don’t want to see other White people in pain and will give them opiates even when it is to their detriment.
The coronavirus is terrifying.
So little is known about the coronavirus. So, Americans are dying. (We do know that washing our hands more often and wearing a face mask is helpful and should be required nationwide, but that is another story.) And we are still learning what happens to those who recover from COVID19. Are there ill effects that may cause long term damage to the lungs, heart, and liver? Time will tell.
But we do know what works to keep opioid addicts alive. We did it before.
Instead of building more prisons to hold drug-addicted Americans, we could treat them. This is nothing new. We did it in the early 20th century. Our policies became irrational and were meant to show how tough the United States could be on dark and brown people. But now, the majority of the victims are white.
We could simply regain the compassion we lost, the care we had in this situation:
“When nonmedical opioid use increased in White communities, rather than arresting consumers, regulators mandated physicians to use Prescription Drug Monitoring Programs, instituted voluntary take-back programs for unused medication, and disseminated the opioid overdose reversal medication naloxone, while passing Good Samaritan laws to protect those calling for emergency assistance during an overdose from drug charges.”
It’s OK. We don’t have to stop progress because of hypocrisy. Let’s just fix the problem, shall we?
1. These programs (Good Samaritan) should be expanded.
2. Allow mandated physicians to use Prescription Drug Monitoring Programs.
3. Stop drug addiction arrests everywhere, and not just in selective white upper-class communities.
4. Use the treatments we have — medical and psychological. We have even more sources at our disposal since the 1920s. But now, like then, we don’t have the political will.
These actions will take the profit out of the drug industry, and empty out our prisons. Since a good proportion of crime is generated because of the need for drugs…that desire would be minimized, and in some cases eliminated.
As a result, there would be a much smaller market.
Many of the people who are dying are lower-middle-class
However, sympathy has been directed towards those from upper-income areas. We can, if we have the will, stop the madness. With the appropriate funding, we can employ social workers and medical staff to the areas that need the help most. They can then put these people into treatment. We must give equal consideration to lower-income areas. Their lives, of whatever color — are of equal value.
The “no drug anytime, anywhere” mandate will not work. It didn’t work in 1914 when the first attempts were made to regulate drugs, and it will not work now. When we see people on a bridge, considering whether to jump or not, we make an effort to save them. This is no different.
Since I started this post some time ago I was informed that opioid overdoses are increasing in the midst of the coronavirus pandemic. Exponentially.
Why won’t we do something about it?
*Mentioned in an 8 February 1914, New York Times article titled “Negro Cocaine ‘Fiends’ Are a New Menace.” by Edward Huntington Williams, M.D
If you or someone you know is struggling with addiction, the Substance Abuse and Mental Health Services Administration can help you locate treatment at www.findtreatment.gov or at this free helpline: 1–800–662-HELP (4357).





