
After COVID-19, Cancer is the Next Thing We Have To Worry About
While we are worrying about COVID-19, we are neglecting routine screening tests for cancer
One man had been having abdominal pain for two months, but he told me he was ‘scared shitless’ of going to the emergency room and contracting COVID-19. He stayed home until he was vomiting and shaking and his wife made him come in. I have another patient who was due for a screening colonoscopy, his first one, but it was delayed a month because the colonoscopy office was closed. He was diagnosed with a large tumor that almost completely blocked off his intestines.
Early on, I predicted that when this first wave of COVID-19 was over, hospitals would see larger numbers of people come in with larger cancers, some possibly causing blockages, some possibly causing bleeding, all causing havoc. This was because I noted that, as people stayed home, and rightfully so, things like colonoscopies and mammograms, deemed non-urgent, fell to the wayside. Federal (CDC) and society guidelines actually urged hospitals to restrict non-essential procedures. This was not wrong at all, it’s just that we will be dealing with the aftermath. I’m a colorectal surgeon, so I’ll focus here on the colonoscopies, though mammograms are no less important.
Fast forward two months, and suddenly we have people who were asymptomatic with cancer and should have been screened but didn’t, or people who were having symptoms (pain, bleeding, weight loss, obstructive signs such as nausea and vomiting) come into the emergency room much sicker than they would have been if they hadn’t tried to stay away due to fears of the coronavirus.
March was National Colorectal Cancer Awareness Month. Usually, this month sees higher numbers of screening than any other month during the year, because of all the health fairs, talks, and social media chatter about it. Did you even see any blue ribbons in your social media feed? No, because it was lost in all the coronavirus panic. In a white paper from Epic, the drop in preventative cancer screenings was between 86–94% (ehrn.org). For colorectal cancer, the weekly average number of screenings fell from 2,895 to 402. Colorectal cancer is the second leading cause of death in the United States; over the last decade, colonoscopy screening has been shown to decrease mortality rates by 20–40%.
Medscape published an article three days ago called “Excess Cancer Deaths Predicted as Care Disrupted by COVID-19”, predicting “33,890 excess deaths among cancer patients in the United States”, 1 year from now. This number includes cancer patients who are particularly susceptible to mortality from SARS-CoV2, but also patients who may lack access to care due to socioeconomic status. The authors noted etiologies such as decreased chemotherapy attendance and lack of urgent referrals as the nation is still conflicted over re-opening.
In April, as the highest daily death rates in New York City were announced, our ventilators and hospital beds were full to capacity with COVID-19 patients. As a surgeon, I could not operate ‘electively’ on a patient who had been diagnosed with cancer because we couldn’t spare the ventilators. Our institutional and societal guidelines told us to refer patients to chemotherapy first, even in cancers that were otherwise operable and should’ve been surgery first. Now, as I see how many people were scared to even go to chemotherapy, I am more concerned than ever.
My offices are slowly opening again with limited hours at the end of May. One month ago I would have warned patients that the risk of contracting COVID-19 was not worth the benefit of going to the emergency room for a simple stomach ache, but now that the daily hospitalizations and mortalities are decreasing, I think that the benefits of seeking medical attention, with appropriate mask and physical distancing precautions, will be worth the risk. Another solution is to offer patients alternative screening methods that they may be able to do at home, ie Cologard stool tests or FIT, a fecal immunohistochemistry test. While the data surrounding these tests as the sole source of screening still do not convey as much confidence as the gold standard colonoscopy. I have to believe that they are better than no screening.
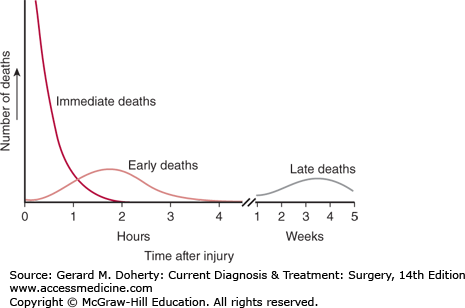
There is a thing that we learn in medical school, called the Trauma Death Graph. While it’s purpose is to show that the majority of people who are treated in the first “Golden Hour” do better, it also shows that there are delayed causes of death, usually due to infection or brain injury. This example has repeatedly popped into my head.
Even as we deal with the deaths from COVID-19, I know that we are going to be dealing with the fallout of this pandemic for years, namely in the form of cancers that didn’t get diagnosed, chemotherapy that was put on hold, and the lack of hospital resources that makes cancer the next thing that we have to worry about.
References