
The Complex Science Behind Convalescent Plasma
Treating of Covid-19 with convalescent plasma comes with its own risks

While simple in theory, the practice of transfusing convalescent plasma to treat Covid-19 is complex and fraught with question marks. Proposing to treat the ill with the blood of the formerly sick is a theory that has been around for well over a century. Even before humans had fully characterized blood, transfusions had already begun to be proposed as a treatment for disease. With the discovery of antibodies, it was theorized that the plasma — the liquid fraction of blood where antibodies live — from people who had recovered from a disease could be used to treat those currently battling the same disease. However, plasma transfusions are not quite so simple.
To understand convalescent plasma, you first need to understand the makeup of blood. Classified as one of the four types of connective tissue in the body, blood is made up of cells, proteins and a fluid matrix that surrounds them called extracellular matrix (ECM). Blood differs from other connective tissues in its percentage of ECM. Many tissues — tendons for example — have relatively small percentages of extracellular matrix making them rigid and dense. Blood on the other had is over 50% ECM making it behave like a liquid. The ECM of blood is known as plasma. Suspended within plasma are the cells that perform most of the vital function of blood — from oxygen transport to immunity. Dissolved within plasma are compounds ranging from nutrients derived from food that are transported throughout the body, hormones secreted to ensure signaling and feedback within the body and a long list of different proteins used to preserve blood volume or aid in blood clotting. Included in that list are antibodies.
Antibodies have played a major role in the narrative around Covid-19 throughout the past six months. Antibodies have a remarkable function in priming the immune system against invasion and in some cases providing outright immunity. The field of biotechnology has harnessed the specificity of antibodies to develop medical treatments and biomedical assays that have revolutionized the field. However, antibodies behave in often unpredictable ways within the body, which is why immunity is not a guarantee for any given disease. It is the unpredictable nature of these immune proteins that has placed them under the spotlight in recent months as researchers question whether antibodies will protect against Covid-19.
Not All Antibodies Are Created Equal
The question of whether or not a viral infection will trigger antibody release in the body is really only the first step in understanding how readily antibodies are made, and whether or not they will be protective. For antibodies to be generated, the host immune system must first recognize a foreign antigen (anti = against, gen = to create). Antigens are essentially molecular signatures on the outer surface of all cells. When foreign invaders are detected, the human immune system employs specialized white blood cells called antigen presenting cells to convey specific antigens to the cells that will begin the antibody response. How vigorously antibodies are generated depends on the antigenicity of the antigen — basically how strongly the body will react to it.
Antigens themselves are highly complex. They are often made up of dozens of different regions that elicit specific responses by host immune systems. These regions — called epitopes — are what antibodies will ultimately bind on to should the pathogen be encountered again. When the immune system encounters a foreign pathogen, it may respond to any, all or none of the epitopes on an antigen. This leads to the production of antibodies that may differ slightly in their structure and function.
The Antigenicity of SARS-CoV-2
The main antigen on the surface of the SARS-CoV-2 virus is known as the s-protein — or spike protein. This protein is a composed of two main subunits, S1 and S2. For the sake of visualization, image the spike protein as an umbrella. The outer surface that fans out away from the virus is the S1 subunit, and the portion that connects S1 to the viral body — like the handle of the umbrella — is the S2 subunit also known as the stalk. Imagining spike proteins as umbrellas is very fitting because functionally the spike protein undulates between different configurations — much like an umbrella goes between closed and open. It is this change in conformation that allows the spike protein to bind on to human cells and begin its invasion.
The movement of spike proteins between different configurations also leads to differing immune response depending on which epitope our immune systems encounter. One research group was able to model the spike protein into “open” and “closed” configurations that correlate with prefusion or fusion of the virus to host cells. Their research demonstrated that antibody generation differed based on the configuration of the spike protein.
Variable antibody response can lead to unpredictable or non-existent levels of protection against Covid-19.
Will Antibodies Protect Against Covid-19?
Circulating antibodies do not always directly correlate with protection against a virus. In the cases of influenza, antibodies are produced during infection, but they confer little protection against a future virus that may have mutated. Even with a virus that is relatively stable genetically, — as SARS-CoV-2 appears to be — the varied antibody response raises the question of whether or not antibodies will actually be protective against the virus.
Some research has found powerful neutralizing capacity in vitro when antibodies isolated from Covid-19 patients are challenged against SARS-CoV-2. These findings raise hopes that immunity from Covid-19 may be possible, whether for those recovering from the disease or those who receive future vaccines.
Yet, immunity remains elusive to so many diseases. In some cases where viruses mutate rapidly, antibodies made from a previous infection are useless against a mutant strain. Such is the case with influenza, whose segmented genome allows for dramatic mutations through a process known as antigenic shift. Luckily, coronaviruses do not have segmented genomes, making their mutation theoretically much slower. In other cases, immunity against a virus simply fades with time. Whether by age, or lack of exposure, antibody levels to certain diseases drop over time. In fact, Covid-19 antibody levels have been show to drop in certain populations of infected persons.
Adding to the complexity of Covid-19 antigenicity is the question of whether the spike protein itself will undergo mutation that allows it to evade existing antibodies. While coronaviruses mutate relatively slow, their receptor binding domains located on the S1 subunit of the spike protein have show mutability. One preliminary report identified the single amino acid mutation D614G as being a factor that not only increased coronavirus’s ability to invade host cells, but in some cases allowed it to resist treatment with convalescent plasma.
Will The Plasma Be A Match
One of the more fundamental problems with convalescent plasma treatments comes down to blood typing. Like any blood product, the antigen profile of donor and recipient need to be matched to avoid adverse reactions. The ABO antigen typing system is the most common way that donor blood is matched with an acceptable recipient. These blood types are based on the presence or absence of antigens on the surface of red blood cells.
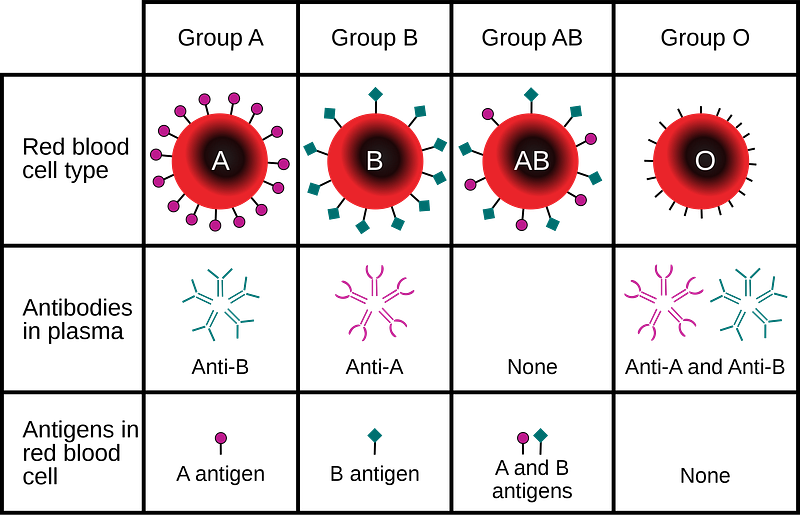
Plasma is matched in a similar way. For example a person with type-A blood has the A-antigen on the surface of their red blood cells, but produces an anti-B antibody in their plasma. Should a type-A person receive type-B blood, their anti-B antibodies would attack the B-type donor red blood cells. When whole blood — meaning all components of blood including cells, plasma, platelets, etc. — is transfused, the blood is matched based on ABO type. Plasma transfusion work almost in the opposite fashion. Type-O blood is considered the universal donor, but Type-O plasma is consider the universal acceptor because it already contains all ABO antibodies that donor plasma might contain. Likewise, a person with type-AB blood has neither anti-A nor anti-B antibodies in their plasma, which means that AB plasma serves as a universal donor because it will not react with recipient blood of any ABO type.
It gets more complicated. Aside from the ABO antigens — along with the rhesus (Rh) antigens that denote the plus or minus on blood types — there are dozens of different antigens on the surface of red blood cells. Kidd, Kell, Duffy and Cromer are just a few of the antigens present on red blood cells. Imagine a person is missing the Duffy antigen on their cells, and then later receives a blood transfusion from a donor who is Duffy positive. The recipient will then develop anti-Duffy antibodies that will then causes a reaction should they ever receive Duffy positive blood in the future. These antigens vary in the severity of reaction that they create, but any mismatch can pose a problem to the plasma recipient.
Many Covid-19 patients face a severe course of injury. Treating a severely ill Covid-19 patient with convalescent plasma runs the risk of an adverse reaction that may worsen their condition. Blood banks keep meticulous records, and transfusions are double, triple and quadruple checked whenever possible. However, blood is often released quickly — as in the case of emergencies — and despite best efforts to provide a match, mismatches do occur. These potential mismatches add yet another level of complexity to convalescent plasma as a treatment for severely ill Covid-19 patient.
While the theory of treating Covid-19 with convalescent plasma is simple in nature, the complexity of human blood transfusions makes it a challenging treatment protocol — especially for the severely ill. Furthermore, the evidence surrounding the protective capacity of anti-SARS-CoV-2 antibodies is still inconclusive, making the convalescent plasma as a treatment experimental at best. As new findings emerge, and research around Covid-19 antibodies develops, convalescent plasma may find itself a tried and reliable treatment for Covid-19. Until then, it remains in question.






{kind=link}
{kind=link}