
Why It’s Almost Impossible to Build a Health Care Startup That Works
And why you should try anyway
We all know the U.S. health care system is bad. But why hasn’t any business come in and fixed it? The market is massive, inefficient, and extremely wasteful. Some estimates suggest wasteful spending accounts for between $760 billion and $935 billion annually, from a combination of unnecessary administrative costs, fraud, over-treatment, poor care coordination, and other factors. It’s an industry ripe for disruption. The challenges created by Covid-19 have added new urgency around fixing the health care system, and will likely inspire a new wave of health tech entrepreneurs. But as someone who has extensively researched health care startups and worked with health care entrepreneurs over the last few years, I have noticed a pattern of challenges that entrepreneurs tend to face as they build health tech companies and try to take on the industry. Here are some of the key issues that make health care particularly tricky to disrupt:
The big obstacles to fixing health care
First, there’s the principal-agent problem, in which the buyer and the user of a good or service are not the same person. For example, most people are on a health insurance plan chosen by their employer. Even though you’re the user, the insurance carrier is selling to your employer, and employers tend to be most concerned about cost. User experience, product simplicity, and other features are a non-priority. Most buyers in health care would rather renew or buy the safest option — they don’t get bonus points for trying a new startup but will get fired if they go with a new startup that fails.
Second, our health care system has evolved to favor customized solutions instead of standardized ones. Each insurer negotiates a different rate for each service at each hospital. Health benefits consultants sell custom benefits packages to each employer. Each hospital uses its own kind of electronic medical record. This lack of standardization makes it extremely hard to scale a health care business because you now need to work around a custom process for each customer, and they expect that level of personalization from their service providers.
Third, health care feedback loops are really long. This makes it difficult to know if your service is working as intended while you wait for feedback, or if in the end it was your service that made the difference. How do you really know it was your therapy solution that helped a patient recover, when it could have been any number of other factors?
Fourth, there’s the employer-insurance entanglement. One of the uniquely terrible things about U.S. health care is that employers get tax-benefitted dollars to pay for health insurance that individuals don’t. This effectively means health insurance is tied to employment, and you switch health plans any time you move or change jobs. Because of that, your insurer has no incentive to keep you healthy long term or give you a great user experience to keep you on their plan, since they know you’re eventually going to switch anyway.
And finally, there’s a huge challenge of getting your first customer. How can you find customers to demonstrate your solution works when no one wants to be the first to try it? Most health care entities want to see some proof before buying. Some companies enter pilot initiatives with hospitals or insurers, but in many cases those are destined to fail as they lack real internal buy-in or resources. There’s a graveyard full of “death by pilot” startups like HomeHero or Healthrageous, where the first customer was used as a case study but didn’t convert into a longer-term relationship.
People new to the business of health care tend to encounter these problems through what I call the “six stages of health tech grief” (my play on Gartner’s Hype Cycle, which illustrates the adoption of new technologies). These are the six stages that many new health startups hit as they try to take on the health care system.
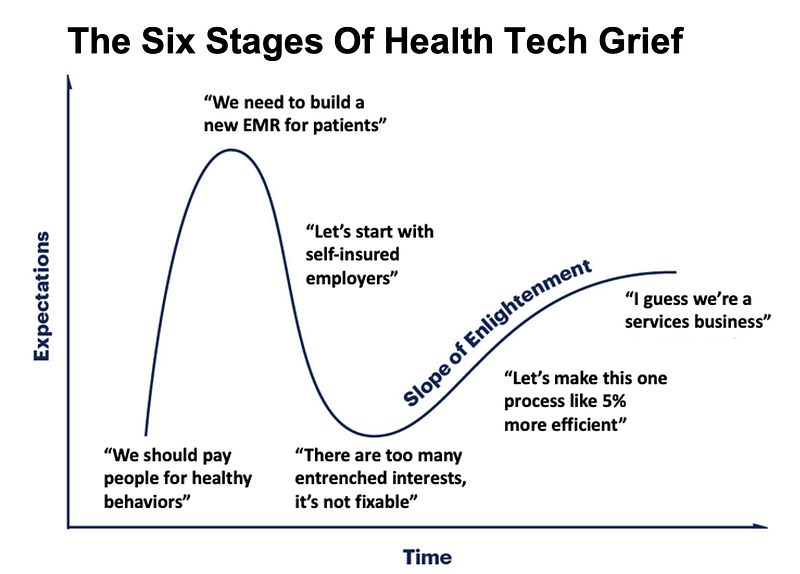
‘We should pay people’
If you were to start disassembling the problems in the U.S. health care system, one of the first things you’ll discover is how much we spend on chronic disease (at least $1.1 trillion in direct costs alone). Many chronic diseases are a result of unhealthy behaviors upstream, so most new health tech entrepreneurs focus on fixing those upstream behaviors.
In the current system, there’s unfortunately no business model to keep someone healthy for the long run.
Poor eating and exercise habits, sleep deprivation, stress, and more lead to a raft of chronic health issues that would be cheaper to prevent than treat over the course of a patient’s lifetime. Wouldn’t it make sense to pay people small amounts today to make healthier choices so we spend less as a system in the long term?

One problem with this approach is that the results of paying people to do different behaviors are pretty mixed depending on the behavior, length of time, and type of reward offered. But the bigger problem is that in the current system, there’s unfortunately no business model to keep someone healthy for the long run. Unless you can lower the cost of some very specific health issue and you can attribute that lowered cost to your specific solution, paying for healthy behaviors isn’t a very attractive proposition.
Giving patients cash for healthy behaviors can work — but it has to be extremely targeted to a specific behavior, and most people who start at this proposition don’t do that. For example, insurance carriers will pay for getting preventive tests like a breast cancer screen, which will save them much more money down the line. It’s also much easier to incentivize a patient to take a one-time preventive test than to fundamentally change their habits.
‘We need to build a new EMR’
Whether or not paying patients for healthy behaviors is a feasible part of your solution, you’ll quickly realize that if you want to build a patient-centric solution, you need patient data, and all the valuable patient data is locked in a disparate network of electronic medical records (EMRs), and it’s hard to get that data out. What we need, you decide, is a new, and better EMR.
Entrepreneurs who try to tackle the EMR problem take one of the following approaches and run into their corresponding challenges:
- Creating a personal health record for patients. The reality is that most patients don’t need to interact with their record very often since they aren’t frequent users of the health care system, so most patients’ willingness to pay for their own record is very low.
- Making a better EMR for doctors. Hospitals and physicians are risk-averse purchasers, and rolling out and training staff on a new EMR can take months, sometimes years. Plus, the reason hospitals buy EMRs is to track the services they bill for, which existing EMRs actually do very well.
- Connecting data from all the existing EMRs. This is a reasonable approach, but it’s a slog and takes a long time. You have to approach each health care provider individually, get an agreement, integrate with them, and then standardize and structure the data. Apple’s Health app is integrated with just 474 health care institutions two to three years after announcing the feature that lets users pull their records in from different health systems. And they’re Apple, not a small startup.
‘Let’s start with self-insured employers’
Employers are even more involved in health care than most people think. Once a company gets to a certain size, it’s likely self-insured. This means that instead of contracting with an insurance carrier, they pay employees’ medical bills themselves, putting them financially on the hook for their employees’ health (for as long as they’re employees of the company).
More than 70 million people in the U.S. are covered by a self-insured plan. Large companies like Walmart, Comcast, and Disney fall into this camp and spend a large chunk of change on their employees’ health care costs. Some entrepreneurs might see this and think, “I’ll bypass the insurance companies by selling directly to these self-insured employers to help them manage their employees’ health.”
Congratulations, you have solved health care.
The problem here is that just 4% of employer plans cover 65% of people in this segment. Given this concentration, those few self-insured employers have heard every pitch already. No employer wants to hear one more pitch from a startup promising to “give your employees telemedicine so they avoid ER visits.” There are a lot of those companies already (98point6, FireFly Health, Teladoc, MDLIVE, to name a few).
Even if you do manage to get a contract with a self-insured employer, you actually have to get their employees to use your product, which is no easy feat. Livongo, a company that helps employees manage their diabetes, says in their investor documents that rolling their solution out takes about three months, and a total of 12 months to get just 34% of total recruitable individuals to use it. And if you don’t get employees to engage, guess who’s not getting a contract renewal?
Let’s make this one process 5% better
Many health tech entrepreneurs eventually decide that the way forward is to narrow their focus to a single pain point of one of their target customers, and make it a little bit better with software.
The idea is that there’s some task or process that’s currently handled with spreadsheets or calls or emails that could be better handled by software. In an ideal world, you would train users to use your software to perform the task, they would see their time spent on the task go down, then the parent company pays you to continue speeding up the task and making their employees’ lives easier. Outside the health care world, for example, a company might integrate Zendesk and Slack to make it easy to see and respond to customer support inquiries. It saves the company time and headache, so they’re willing to pay for these tools.
When you say “our tool can do this for you” the other side is hearing “here’s another thing you have to learn after you spent months trying to figure out the last tool.”
There are a few reasons I think this is way tougher in health care.
What you think is a lightweight tool that can plug nicely into some process without integrating with too many systems is never as lightweight as you think. Most health care companies have dragged their feet on moving their IT infrastructure to the cloud and have rigorous compliance processes which they evaluate their vendors against. If you need to pass data between any two systems, this is going to take time from both you and your customer to get up and running.
And then we’re back to the principal-agent problem. The person making the purchasing decision and the person using the product are totally different. At a hospital, the purchaser might be a chief information officer, but the user would be frontline physicians. The CIO cares way more about keeping price and workflow disruption to a minimum than making marginal improvements to usability or the speed of doing things.
The other unfortunate reality is that no one in health care wants to learn a new tech tool or process. When you say “our tool can do this for you” the other side is hearing “here’s another thing you have to learn after you spent months trying to figure out the last tool.”
When you try to sell software tools for a specific use case, you’ll also discover that the companies you’re selling to actually can’t use the tools properly because they either don’t have the expertise in-house (for example, data/tech talent or health care knowledge), or because the efficiencies you created with your tool immediately get wiped out once you hit whatever the legacy system is.
Many entrepreneurs either end up having to loan people out to help their clients make the most of their tool — or realizing that it makes more sense to actually become a tech-enabled pharmacy, insurance carrier, or provider themselves.
‘I guess we’re a services company’
Trust is the most valuable currency in health care. To earn that trust, some companies will tie themselves to outcomes, that is, only get paid if the product works. But to ensure that the buyer uses the product effectively, many companies eventually realize that they need to move beyond just software and include services as part of their sale.
Many tech companies discover that services are actually a great way to help scale their business. Digital health companies will use professional services to help onboard, train, and set up a company onto their platform. Companies like Veeva and Health Catalyst have done this well.
Services can also be the core product, with tech living in the background to help it scale. Livongo is a good case of how delivering on outcomes for their customers let them expand into new areas. It started by helping employers manage their employees with diabetes via remote monitoring, coaching, texting, and emails. But their success in that area is what let them expand into other chronic disease areas (such as hypertension).
You can use tech to streamline your operations too. One Medical, a primary care company, is leaning heavily into digital visits, which would be way cheaper and more scalable for them operationally. Physicians can “see” more patients asynchronously via text, use lower-cost labor when possible, and fill unused capacity when the physicians have downtime in-office.
Do you need to be a services company to be successful in health care? No. Many companies build solid businesses by sticking to software, but many of them see their revenue growth slow quickly as they find it difficult to scale past their initial few customers. So there’s nothing wrong with having a higher headcount to support services — it potentially means bigger contracts, smoother operations, and more, if you do it right.
Why you should still build a health care company today
Even though I just explain all the mistakes and challenges a new health care-focused tech startup would face — I still think this is the best time ever to build a health care company.
Thanks to the cloud, new plug-in services designed to help health tech companies, and better hardware, the infrastructure needed to build a new health care startup has never been better, and continues to improve. New regulations are making it easier to get paid, share data, and deliver care virtually. Meanwhile, incumbent companies are stuck in their old business models and processes.
Health care is hard, and I can’t pretend like it isn’t. But if you can navigate through the challenges, you can build an extremely valuable business that tangibly improves the lives of people.




